
THE ALIGNMENT BETWEEN SELF-REPORTED AND
ADMINISTRATIVE MEASURES OF APPLICATION TO AND RECEIPT OF
FEDERAL DISABILITY BENEFITS IN THE HEALTH AND RETIREMENT STUDY
Jody Schimmel Hyde and Amal Harrati
CRR WP 2021-26
December 2021
Center for Retirement Research at Boston College
Hovey House
140 Commonwealth Avenue
Chestnut Hill, MA 02467
Tel: 617-552-1762 Fax: 617-552-0191
https://crr.bc.edu
Jody Schimmel Hyde is a principal researcher and deputy director at Mathematica’s Center for
Studying Disability Policy. Amal Harrati is a researcher at Mathematica. The research reported
herein was pursuant to a grant from the U.S. Social Security Administration (SSA) funded as
part of the Retirement and Disability Research Consortium. The findings and conclusions
expressed are solely those of the authors and do not represent the views of SSA, any agency of
the federal government, Mathematica Policy Research, or Boston College. Neither the United
States Government nor any agency thereof, nor any of their employees, makes any warranty,
express or implied, or assumes any legal liability or responsibility for the accuracy,
completeness, or usefulness of the contents of this report. Reference herein to any specific
commercial product, process or service by trade name, trademark, manufacturer, or otherwise
does not necessarily constitute or imply endorsement, recommendation or favoring by the United
States Government or any agency thereof. The authors wish to acknowledge outstanding
programming work by Rachel Hildrich as well as valuable review comments from Purvi Sevak
and Michael Anderson, all of Mathematica. Additionally, this work benefitted from discussions
about the HRS-SSA linkage with David Weir and Chichun Fang at the University of Michigan.
© 2021, Jody Schimmel Hyde and Amal Harrati. All rights reserved. Short sections of text, not
to exceed two paragraphs, may be quoted without explicit permission provided that full credit,
including © notice, is given to the source.
About the Center for Retirement Research
The Center for Retirement Research at Boston College, part of a consortium that includes
parallel centers at the National Bureau of Economic Research, the University of Michigan, and
the University of Wisconsin-Madison, was established in 1998 through a grant from the U.S.
Social Security Administration. The Center’s mission is to produce first-class research and forge
a strong link between the academic community and decision-makers in the public and private
sectors around an issue of critical importance to the nation’s future. To achieve this mission, the
Center conducts a wide variety of research projects, transmits new findings to a broad audience,
trains new scholars, and broadens access to valuable data sources.
Center for Retirement Research at Boston College
Hovey House
140 Commonwealth Ave
Chestnut Hill, MA 02467
Tel: 617-552-1762 Fax: 617-552-0191
https://crr.bc.edu/
Affiliated Institutions:
The Brookings Institution
Mathematica – Center for Studying Disability Policy
Syracuse University
Urban Institute
Abstract
This paper examines the alignment between self-reported and administrative records of
applications to and receipt of federal disability benefits. It uses data from the Health and
Retirement Study (HRS), specifically the cross-wave consistent version developed by the RAND
Corporation. The HRS has surveyed adults over the age of 50 every other year since 1992 to be
nationally representative of the non-institutionalized older adult population, replenishing the
sample with a new cohort every six years. The HRS asks respondents periodically if they are
willing to have their survey information linked to earnings and benefits information maintained
by the U.S. Social Security Administration (SSA). Most respondents agree to the linkage, which
provides another source of information about application and receipt patterns for Social Security
Disability Insurance (SSDI) and Supplemental Security Income (SSI) than the data that is
collected from respondents in the survey. This information may be valuable in understanding
disability program participation among older workers and the extent to which survey respondents
accurately report their benefit receipt.
Using information in the HRS linked to SSA’s Form 831 records about disability benefit
applications and its Disability Analysis File about benefit receipt, the paper compares survey and
administrative reports of having ever applied to SSDI and SSI as well as the receipt of those
benefits in each HRS survey wave from 1996 through 2016. It presents statistics on the
characteristics of HRS respondents based on whether they consented to have their records linked
to administrative files as well as whether those who consented to the linkage accurately reported
their benefits status. The analyses make comparisons by calendar year and HRS sampling
cohort, as well as by each age from 51 through full retirement age. An appendix to the paper
offers a primer for other researchers considering using the HRS-SSA linked data.
The paper found that:
• Older cohorts in the HRS are more likely than younger ones to have consented to having
their HRS data linked to SSA administrative records. Younger cohorts, however, are
more likely to have consented in recent years, which is necessary to have been included
in HRS’s prospective permission scheme and to have consented to certain file linkages
that may be useful to researchers, including the ones we used in our analysis.
• Aggregate self-reported percentages of application and receipt of SSDI and SSI are lower
than those reported in HRS-SSA administrative data at nearly all ages, but rates of new
applications and receipt of benefits (i.e., incidence) are similar between the ages of
entering the HRS survey (51-56) through SSA’s full retirement age.
• There are differences in SSDI and SSI application and receipt shares between HRS self-
reports and administrative data across birth cohorts in the survey, but no systematic
pattern in the difference between the two sources of information across all of the survey
cohorts.
• Individual misreporting represents a minority of total cases but is more common relative
to the share of older adults with interactions with the SSDI and SSI programs. Misreports
range from approximately 4 percent to 12 percent of total respondents, depending on the
program and age of respondents. False negatives (the respondent reports no application
or receipt while the SSA data indicates application or receipt) tend to be more common
than false positives, especially at older ages.
• The demographic, socioeconomic, and health characteristics of respondents who
incorrectly report their benefits receipt (relative to SSA information) are different from
respondents whose self-reports align with administrative records. Those differences vary
by receipt of SSDI or SSI, but include respondent age, race, income, assets, education,
health conditions, and health behaviors.
The policy implications of the findings are:
• Researchers who use HRS self-report data alone should be aware of differences in the
prevalence rates relative to SSA-published statistics and administrative records for the
same respondents. Using HRS self-reported data is likely to result in an underestimation
of program application and receipt relative to HRS-SSA data. Moreover, characteristics
of those who misreport differ from the full sample, meaning that descriptions of
applicants’ or recipients’ demographics, employment, income, and health may differ
depending on what sample is being used. As such, care should be taken in interpretations
of applicant or beneficiary characteristics when using self-reports.
• Use of the SSA data linkage may not be feasible for all research purposes, particularly
those where a loss in sample size due to consenting to the linkage would be problematic.
In cases where a linkage may not be practical, use of self-responses can still be
informative in many research applications. These can include, but are not limited to,
longitudinal analyses of employment or health characteristics in relation to SSA
programs or the use of receipt or beneficiary status as covariates or controls in analysis.
Introduction
Understanding the circumstances that lead to federal disability benefit application and the
post-application outcomes of both beneficiaries and denied applicants is critically important for
considering changes to the determination process, program rules, or benefit generosity. The
Social Security Administration (SSA) only collects information necessary to make benefit
determinations and administer monthly benefits. As such, SSA collects some information from
applicants about their work history, education, health status, income, and assets, but does not
always know with whom applicants live, their other income sources, and whether they receive
other forms of public or private assistance (SSA 2021). Once receiving benefits, SSA may
periodically collect information on an individual’s health status for the purposes of continuing
disability reviews and will know if participants’ earnings exceed substantial gainful activity, but
the information available to the agency is limited.
For these reasons, researchers and policymakers turn to other sources information
collected from disability program applicants and beneficiaries to have a more comprehensive
understanding of their needs. Many nationally representative surveys collect detailed
information from their respondents, including whether they believe they have a disability, have
applied for Social Security Disability Insurance (SSDI) or Supplemental Security Income (SSI),
or receive benefits from either program. Many of these sources solely collect self-reported
information from their respondents, but some surveys link information collected from survey
respondents to the SSA’s administrative data to augment self-reported benefits status with the
best information available to the agency. Recent research has capitalized on that linkage to
better understand the accuracy of self-reported survey data, which is critical both in deciding
how much trust to place in self-reports, but also in considering how to combine information from
two potentially differing sources. As we discuss in what follows, the findings vary by the source
of public benefits as well as the survey collecting the data (see for example, Meyer and Mittag
2019; Chen, Munnell, and Sanzenbacher 2018; Bee and Mitchell 2017).
In this manuscript, we compare reports of SSDI and SSI application and receipt using
survey data from the Health and Retirement Study (HRS) to similar information contained in
SSA administrative records. The HRS is a nationally representative, longitudinal survey of
noninstitutionalized adults in the United States from age 51 onward that started in 1992; each
respondent is interviewed every other year until they die or otherwise exit the study. As
2
respondents age, the HRS replenishes the survey every six years (in 1998, 2004, 2010, etc.).
During each survey wave, respondents report their own benefits history, but have been
periodically asked to have their information linked to earnings and benefits information stored by
SSA, which administers the federal disability programs. Not all survey respondents consent to
the linkage, but for those who do, it is possible to compare information reported by respondents
to their administrative record to better understand the validity of self-reported benefits status and
the potential utility of the administrative linkage for research purposes.
There are several reasons why making such a comparison with the HRS is important,
even with the extant literature from other survey data sources. First, health shocks occur more
frequently with age (Smith 2003), so HRS respondents will have heightened need for federal
disability benefits relative to younger adults in other national surveys. Second, the years just
before retirement offer what might be a potentially confusing mix of benefits: SSDI is available
through full retirement age, Old Age and Survivors Insurance (OASI) benefits become available
at age 62, and SSI benefits span both ages with eligibility requirements that change at age 65.
Thus, misreporting may be more common, particularly given that all three programs are
administered by SSA. Finally, the HRS has been collected since the early 1990s, and since that
time, survey nonresponse has increased (Singer 2006), which could also signal changes in the
quality of information obtained from those who do participate. Understanding how responses to
questions on disability benefits and consenting to the administrative linkage over subsequent
cohorts in the HRS may help researchers select samples and frame questions for future research
studies.
Our descriptive analysis is meant to provide information to HRS users about the accuracy
of self-reported disability benefits collected in the survey and the potential strengths and
limitations of using the matched administrative data. We answer the following questions:
• What share of HRS respondents consented to having their data linked to allow for the
measurement of SSDI and SSI application and receipt? How did the likelihood of
consenting vary by cohort and over time?
3
• How do HRS respondents who consented to the SSA administrative linkage differ from
those who did not, in terms of characteristics and the reporting of SSDI and SSI
application and receipt?
• How do prevalence rates of having applied for or received SSDI or SSDI vary by cohort,
time, and age? How different are the aggregate rates if a researcher were to use the self-
reported data instead of the administrative records, and what factors might explain the
difference?
• Among respondents who consented to the linkage, how accurate are self-reports, and
what do we know about respondents whose reports are incorrect?
We find that a majority of HRS respondents have consented to having their data linked to
SSA records, but rates of consent differ by survey cohort and over time. Consistent with earlier
studies, we find demographic, employment, and health-related characteristics differ between
respondents who do and do not consent to the linkage. We also find that generally, the share of
respondents who report having applied to or receiving SSDI or SSI is lower than SSA records
indicate. The pattern of underreporting is generally consistent across respondent age (regardless
of what cohort or survey year they are asked); however, there is not a consistent pattern across
survey cohorts. As with consenting to a linkage, we find differences in demographic,
socioeconomic and health characteristics for respondents whose self-reports are discordant from
their administrative records as compared to those who do not misreport.
In addition to documenting the alignment between self-reports and administrative
records, this manuscript contains a primer for other researchers interested in using the HRS
linked administrative records (Appendix A). While the SSA linkage has been available for more
than two decades, using it requires detailed knowledge of the administrative files and the HRS
process for collecting consent from survey respondents to link their data. With these high
barriers to entry, the SSA linkage has potentially been underutilized. Our hope is that the
manuscript combined with the primer will facilitate use by a broader array of researchers,
particularly for research projects where the richness of the administrative data opens up new
research possibilities to understand longitudinal outcomes of disability applicants and
beneficiaries.
4
Background: The Accuracy of Self-Reported Public Benefits in National Surveys
Surveys offer a depth of information not available in administrative sources alone. This
is especially true for longitudinal surveys, which can provide a detailed look at the
characteristics, outcomes, and trajectories of individuals before, during, and after they apply for
or receive SSDI or SSI. Davies and Fisher (2009) document some of the potential uses of linked
survey and SSA administrative data, while also offering a succinct assessment of earlier work by
researchers including Hyunh et al. (2002) and Koenig (2003) to document the reporting of SSDI
and SSI in survey versus administrative sources. They summarize the literature based on
analysis of data from older adults in the 1990s as showing that respondents to the Current
Population Study (CPS) slightly underreported OASDI and significantly underreported SSI
benefits, while the Survey of Income and Program Participation (SIPP) slightly overreported
OASDI income and was mixed on SSI. Schimmel Hyde et al. (2018) used 2008-2009 data from
the same sources and a working-age population and found that relative to the administrative
record, many beneficiaries misreported their benefits status and income from benefits, and that
discrepancies appeared to be larger than in earlier years of the surveys.
Recent research has sought to augment self-reports in surveys to understand the income
from public benefits more broadly. Beginning with Meyer et al. (2015), together they suggest
that misreporting is not uncommon and errs toward underreporting rather than overreporting.
Meyer and Mittag (2019) found that income from public programs among working-age
respondents in the CPS were dramatically understated in the CPS. Bee and Mitchell (2017)
similarly documented underreporting of income among older adults in the CPS, driven primarily
by misreported defined benefit pensions and retirement account withdrawals. Chen et al. (2018)
extended the Bee and Mitchell work to other data sources and found that the CPS was an outlier
in terms of retirement income misreporting. Compared to capturing 61 percent of retirement
income in the CPS, the SIPP, for example, captured 93 percent of retirement income relative to
administrative data, while the HRS captured 96 percent.
Despite the linkage to SSA administrative data for two decades, to our knowledge, there
has not been work to date to understand the accuracy of reports from HRS respondents about
applications to and receipt of SSDI and SSI. Our paper compared self-reports to administrative
records. While it is simplest to assume that deviations between the two sources reflect
respondent misreporting, it is important to note that there are reasons that individual reports may
5
offer more current or complete information than the administrative records. We will discuss
reasons for deviations in what follows, in part to couch our findings, but also so that other
researchers can use assess the strengths and limitations of self-reports relative to administrative
data based on the research question at hand.
Data and Measures
In this section, we describe the data sources in more detail, the sample cohorts that we
include in our analysis, and the measures we use to document SSDI and SSI application and
receipt. We also discuss the process to collect consent for the administrative linkage from HRS
respondents, implications for sample size, and our approach for adjusting the sample weights to
account for non-consenters.
Data Sources
We combine information from publicly available survey data from the HRS with
restricted-access SSA administrative records. The latter are available with permission from the
HRS following an in-depth application and review process. We focus on a high-level discussion
of the four sources of data we use in our analysis here; more detailed information about the files
and the construction of our measures is contained in Appendix A.
The RAND-HRS is a cross-wave consistent file of the HRS, developed to facilitate
research. The HRS is a longitudinal survey that is nationally-representative of the
noninstitutionalized population in the United States over the age of 50. It has been fielded
biennially since its introduction in 1992. The survey is known for its richness of data on health,
income, retirement, and other topics important to older adults. The RAND-HRS simplifies
information collected about SSI and SSDI benefits over many years of the study and using
different survey instrument design, but is solely based on respondent self-reports in the HRS.
For our analysis, we use the version of the file that contained data through 2018.
Form 831 Respondent Records is an SSA administrative file that contains information on
initial applications for SSDI and SSI. The file we use contained data from 1988 (when SSA
began storing the information) through 2016. Form 831 records are limited to initial applications
that received a medical review and do not include initial applications that were denied because
they did not meet the financial criteria of federal disability programs, nor appealed applications.

6
The Disability Analysis File (DAF) is an SSA file that combines data from multiple
administrative sources to produce monthly information about the receipt of SSDI and SSI
benefits starting in 1996. The version of the file we use contained data through 2018.
The HRS-SSA Permissions Consent History is a file available from HRS that provides
information about whether a respondent to the HRS consented to having their information linked
to SSA records and whether a match with the data was found. We use this file to determine
which respondents might have information available on disability program participation in the
administrative records.
Sample Selection
To align with the availability of administrative records, we use data from 1996 through
2016, spanning four cohorts of the HRS. The cohorts include the HRS cohort (first interviewed
in 1992; birth years 1931-1941), War Baby Cohort (first interviewed in 1998; birth years 1942-
1947), Early Baby Boomers (first interviewed in 2004; born 1948-1953), and Middle Baby
Boomers (first interviewed in 2010; born 1954-1959).
1
We include age-eligible sample members
in each cohort, meaning that younger spouses who were interviewed with an older age-eligible
respondent are included in our analysis once they themselves age into the survey. Except for the
initial HRS cohort, these cohorts were first interviewed when they were ages 51-56. The HRS
cohort included more birth years than the others; for parallel construction with the other later
cohorts, we include only the “young HRS” born in 1936-1941 and first interviewed at ages 51-56
in 1992. We refer to this as the HRS cohort in what follows for simplicity; it is important to note
that we found that the younger and older birth years of the HRS cohort differed in the outcomes
considered in this manuscript.
For three of the cohorts, we use the data collected every other year from the initial
interview through 2016 (Table 1). The exception is the HRS cohort, which initially was
surveyed in 1992, but we do not include in our analysis until 1996, to align with the availability
of data on disability receipt from the DAF. Once the individual reaches SSA’s full retirement
1
The Late Baby Boomers (born 1960-1965) were first interviewed in 2016, but we exclude them from our analysis
because they only had one wave of data during our analysis.

7
age, we no longer measure their SSDI or SSI status.
2
For the birth years in our analysis, SSA was
gradually increasing the FRA from 65 to 66; it was under age 66 for those born before 1943
(increasing by 2 months from 65 to 665 gradually), exactly 66 years for those born from 1943
through 1954, then again increasing gradually to age 67 for those born later. In our cohort
analysis, we categorize respondents in each wave into four groups (1) interviewed, (2) not
interviewed (but alive), (3) dead (but not yet FRA), and (4) interviewed, but reached FRA.
2
At FRA, SSDI benefits convert to Social Security retirement benefits automatically. SSI benefits transition from
disability to old age at age 65, but for purposes of aligning the cohorts, we counted them through FRA; we discuss
the implications of this decision in the results section.
8
Table 1. Timing of HRS Cohort Entry and Interview Waves Used in Analysis
HRS Survey Wave
Birth year
1992
1994
1996
1998
2000
2002
2004
2006
2008
2010
2012
2014
2016
HRS
1936-1937
X
57-58
59-60
61-62
63-64
65-66
1938-1939
X
55-56
57-58
59-60
61-62
63-64
65-66
1940-1941
X
53-54
55-56
57-58
59-60
61-62
63-64
65-66
War Baby
1942-1943
X
57-58
59-60
61-62
63-64
65-66
1944-1945
X
55-56
57-58
59-60
61-62
63-64
65-66
1946-1947
X
53-54
55-56
57-58
59-60
61-62
63-64
65-66
Early Baby Boomer
1948-1949
X
57-58
59-60
61-62
63-64
65-66
1950-1951
X
55-56
57-58
59-60
61-62
63-64
65-66
1952-1953
X
53-54
55-56
57-58
59-60
61-62
63-64
Middle Baby Boomer
1954-1955
X
57-58
59-60
61-62
1956-1957
X
55-56
57-58
59-60
1958-1959
X
53-54
55-56
57-58
Note: X indicates the first wave the cohort was interviewed by the HRS, at ages from 51-56. Shaded cells indicate the survey waves from which we used data
from each cohort. The value shown in each cell is the approximate age range of the birth cohort during the survey wave.

9
HRS Consent Requirements and Implications for Sample Selection
The SSA administrative linkage to the HRS is only available for respondents who
consented to having their records linked and who provided the requisite information to facilitate
a linkage (accurate Social Security number, name, date of birth, and gender). The consent
process has changed over the years of the HRS, as described in more detail in Appendix A.
Importantly for our analysis, the SSA 831 files and DAF are available only for respondents who
consented to the linkage in 2006 or later, meaning that earlier cohorts had the opportunity to
initially consent, but may not have provided the requisite permissions to be in our analysis of
administrative data.
Table 2 shows the full unweighted sample size for each cohort in our analysis, as well as
the share of each cohort who consented to the linkage to SSA benefits data, ever and in 2006 or
later. Over time, the share of each cohort consenting to any linkage has declined, from 88.0
percent in the HRS cohort down to 78.6 percent of Middle Baby Boomers. Despite the declining
rate of consent, the rate of consenting in 2006 or later increases across the cohorts, from 49.0
percent among the HRS cohort to 77.4 percent of the Middle Baby Boomers. The lower rate in
earlier cohorts reflects the fact that those cohorts had a longer elapsed time from survey entry
through 2006, over which many of the respondents left the sample, died, or did not reconsent. In
what follows, we refer to sample that consented in 2006 or later the “consenter sample” for ease
of terminology, noting that this excludes those who consented in an earlier year. Appendix
Table B.1 provides more detail on the interview and consent status of each cohort by birth year
and HRS wave.
Table 2. Sample Size of Each HRS Cohort, by Consent Status
Number of
respondents
Never
consented
Consented
pre-2006
a
Consented
2006 or later
Share ever
consenting
to linkage
Share with
2006 or later
consent
HRS
5,604
670
2,186
2,748
88.0
49.0
War Baby
3,090
473
656
1,961
84.7
63.5
Early Baby Boomer
3,369
578
449
2,342
82.8
69.5
Middle Baby Boomer
4,782
1,019
59
3,703
78.6
77.4
a
Some of the sample members in the Early Boomer and Middle Boomer cohorts were initially interviewed as
younger spouses of respondents in earlier cohorts. We included these respondents based on their own birth year
cohort, but they were able to provide consent to the linkage before their birth year entry cohort while in the same as
an age-ineligible spouse.
Source: Authors’ calculations using the RAND-HRS and SSA data linkage. Sample sizes are based the age-eligible
cohort at survey entry year and do not include age-ineligible spouses or spouses added in subsequent survey waves.

10
Consistent with earlier work (HRS, March 2021), we found that the consenter sample has
different characteristics than the full HRS sample (Appendix Table B.2). In brief, we find that
respondents who consent to linkage are more likely to be white, female, and employed, have
higher education, longer work histories, and lower rates of chronic conditions including heart
disease, lung disease, diabetes, and stroke. Consenters report lower rates of smoking and
drinking, fewer difficulties with activities of daily living (ADLs) and fewer hospital stays and
doctor’s visits.
Weighting
Because of the differences in the sample size and composition between those that consent
and the full HRS sample, simply using the administrative linkage with the HRS survey weights
will not produce nationally representative estimates. To adjust the sample weights, we predicted
the likelihood of consenting in 2006 or later using a logistic regression in each survey wave
following a process that the HRS uses. Our model included sex, race and ethnicity (indicators
for Black and Hispanic), marital status (indicators for married, divorced, and widowed),
education (indicators for high school graduate, some college, college graduate or advanced
degree), an indicator for being employed, categories of self-rated health status, and quintiles of
household income and wealth.
3
We used the predicted values from the logistic regression models to generate inverse
probability weights (IPW), which we then applied along with the HRS sampling weights to the
consenter sample. Applying the IPW in each wave to the survey weights yields a weighted sum
of interviewed consenters in each wave that equals the weighted sample size of interviewed
respondents that wave from the full HRS.
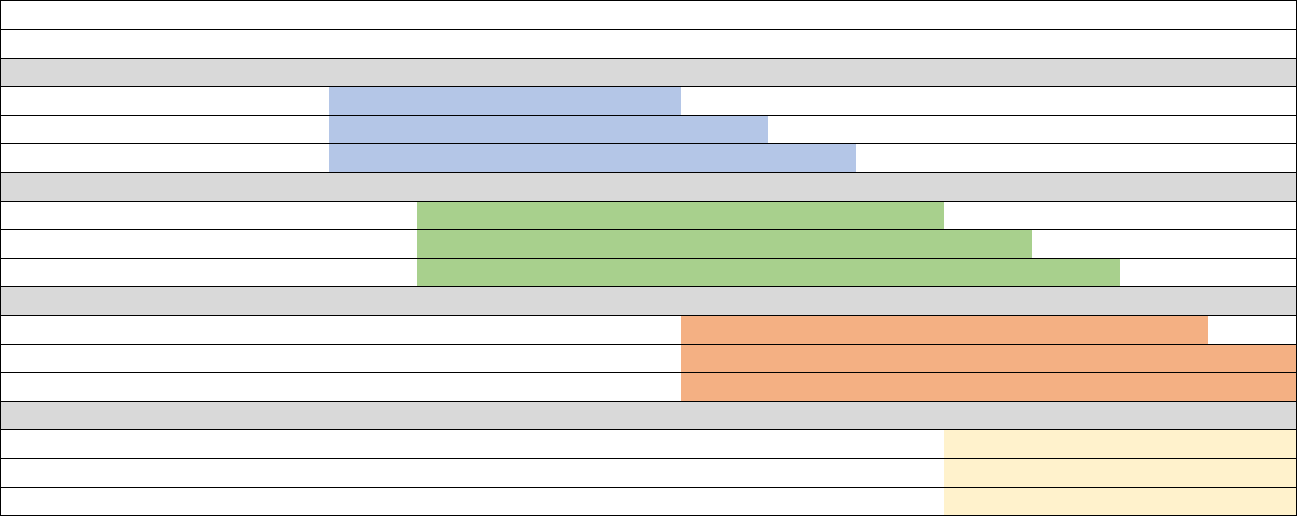
Figure 1 shows the weighted distribution of each cohort and wave, from the year of
entering the survey through 2016, applying the wave-specific IPW to the baseline weights for
each cohort. In the figure, gray bar shows the number interviewed in each wave who had the
necessary consent to be in the SSA administrative files we use. The IPW reweighting process
for analyzing the administrative data means that the weighted sum of the consenter sample (gray
3
We used the same characteristics to predict the likelihood of consenting in 2006 or later as the HRS uses to
construct its wave-specific weights for working with the SSA data. In our case, we needed to modify their process
for some of the analyses that follow and could not solely rely on the weights they developed consents. We used
cross-wave consistent measures of the included variables from the RAND-HRS file.
11
portion of the bar) equals the weighted sum of the total number interviewed in each wave (the
combination of the light blue, orange, and gray bars). Over time, the share of the sample that is
interviewed falls due to attrition or death. The full HRS and War Baby cohorts reach FRA
before 2016, while only part of the Early Baby Boomers do (and none of the Middle Baby
Boomers). Because two-year birth cohorts attain FRA over multiple survey waves, it is
important to note compositional changes in the “cohort” included in our analysis in the years
approaching FRA, as shown in Table 1.

12
Figure 1. Interview and Consent Status of Each HRS Cohort from 1992 through 2016
Notes: Values are weighted using the HRS sampling weight from the baseline interview in each cohort. Analogous unweighted values are contained in Appendix
Table B.1.
Source: Authors’ calculations using the RAND-HRS and SSA data linkage.
13
Measuring SSDI and SSI Application and Receipt
In this section, we describe our approach to measuring applications to and receipt of
SSDI and SSI; more details are contained in Appendix A. Self-reported values are defined using
cross-wave consistent measures in the RAND-HRS file. Administrative information on
applications came from SSA’s Form 831 records, as linked to the HRS, while administrative
records on benefit receipt were derived from the DAF. If an HRS respondent consented to the
SSA linkage but did not have information available in the 831 file for either SSDI or SSI, we
assume they had not applied for benefits. We follow a similar approach if they consented to the
administrative linkage but did not have a record in the DAF, coding the respondent as a non-
beneficiary (for the relevant program).
Application. For self-reported applications, we use the spell data available in the RAND-
HRS to identify whether the person had ever reported applying for SSDI and/or SSI by the date
of the HRS interview. We measure applications in SSA administrative records using Form 831
records, which contain information on initial disability applications from 1988 onward. For both
the self-reports and administrative data, we assume that if the respondent is a beneficiary (based
on the comparable self-report or administrative measure), that they applied for the program at
some point in the past, even if the application data do not indicate that to be the case. This is
especially important in the administrative data because the 831 records began in 1988. It is
therefore quite likely that sample members in the older cohorts might have applied for and begun
to receive benefits before that time; we would observe them as receiving benefits but might not
find their application in the 831 files. It is also possible that HRS respondents may have
neglected to provide complete application data for spells that began long before their first HRS
interview, despite accurately reporting current receipt data.
As described in more detail in Appendix A, there are reasons why individual self-reports
of applications may not align to administrative records. Most importantly, the 831 records likely
undercount what individuals themselves would report, because the former only contain
applications that have received an initial determination following a complete medical review by
SSA’s Disability Determination Services offices. The 831 file does not include (1) applications
that have not yet received an initial determination, (2) applications denied on the basis of not
meeting the program’s financial criteria, and (3) applications being appealed beyond the initial
and reconsideration levels. Based on the questions in the HRS, all three of these scenarios would

14
be reported as an application by respondents. It is also possible that the 831 file contains
applications that respondents may not report; for example, a respondent who applies for SSI may
not know that SSA will also process an application for SSDI if eligible.
Benefit Receipt. We measured the receipt of SSDI and SSI at time of the HRS interview.
For self-reports, we used wave-specific measures in the RAND-HRS indicating that the
respondent was currently receiving benefits from SSDI and/or SSI. We measured the receipt of
benefits based on SSA administrative records using the DAF. We measured benefit receipt in
the DAF based on beneficiaries being in current payment status in the month(s) of the HRS
interview.
4
One important consideration in our measures of benefit receipt is that the HRS question
wording in the earlier years allowed for uncertainty in program participation in a way that did not
occur in later waves. From 1992 through 2000, respondents were asked about SSDI and SSI
together. Where possible, information collected from respondents after 2000 was subsequently
used to “backfill” records by RAND in the cross-wave consistent measures in the RAND-HRS
for each program (e.g. replacing “SSDI or SSI” with “SSDI but not SSI” based on later reports).
It was not possible in all cases (for example, if a respondent died or left the sample), and prior to
2000, so a fair amount of uncertainty remains about the program under which respondents
applied for or received benefits. After 2000, the survey questions on disability benefit receipt
were separated by program.
To be the most consistent across time, we opted for a “narrow” measure in which we did
not account for application/receipt from an unknown program, limiting our applicants and
beneficiaries only to those for whom definitive information about the program was available.
(For example, respondents who did not ever clarify whether they received benefits from SSDI or
SSI were classified as not being beneficiaries.) Based on our review of patterns over time, the
narrow measure we use likely understates program participation before 2000.
5
4
In cases where the HRS interview spanned multiple months, we looked for benefit receipt in any of those months
in the administrative data.
5
In the earliest years of the survey (1992 and 1994), many of the application and receipt reports were not reconciled.
SSDI application and receipt prevalence rates that included the unknown program category were 2-3 times higher
than those we report, and SSI application and receipt rates that were 7-10 times higher. The magnitude of the
difference got smaller in each year through 2000, presumably reflecting a higher likelihood of reinterviewing
respondents in 2000 or later that allowed for the record to be updated.
15
Profiles of SSDI and SSI Application and Receipt by Time and Cohort
To start, we consider the aggregate alignment of survey and administrative reports in
each year, incorporating all four of our cohorts. In general, self-reported applications to and
receipt of SSDI and SSI are lower than comparable administrative reports. However, the rates of
new applications and receipt over time are quite similar. Figure 2 shows the profile of each of
the four measures of interest in each HRS interview year from 1996 through 2016 for the cohorts
included in our analysis. The black line shows self-reports, while the gray line shows
administrative values, where both have been weighted to be nationally representative; the former
using HRS sampling weights and the latter using the IPW method above to reweight the
consenter sample to the same overall population size.
Starting with SSDI, we see that both self-reported and administrative measures of receipt
generally increase over the period. Self-reported values of receipt are always lower than the
measure using administrative data at the same time, with the former increasing from about 2
percent in 1996 to just under 10 percent in 2016 and the latter increasing from 7 percent to just
over 10 percent over the same period. The share who had ever applied for SSDI at each point is
lower based on self-reports than administrative records through 2004, almost identical through
2008, after which the self-reports are higher than administrative values. Self-reports start with
around 4 percent reporting having applied for SSDI in 1996 and rise to 16 percent by 2016, while
administrative records show about 8 percent had applied by 1996 and 14 percent by 2016. The
patterns over time are consistent with increasing SSDI receipt over the period, though the
addition of new, younger cohorts in 1998, 2004 and 2010 obscure some of the patterns of the
aging of the earlier cohorts. The youngest cohort was 51-56 in 2010 and had aged 6 years by the
last year, showing an application and receipt pattern consistent with increased SSDI receipt with
age.
Despite level differences in SSDI receipt and application in self-reports and
administrative data, both sources show similar patterns in new receipt and applications over the
period. The slopes of the lines measure new receipt and/or application and are therefore
analogous to incidence of program application or participation. The slopes of the lines for SSDI
receipt are relatively similar at most points after 2000 (when the HRS began asking separate
questions about SSDI and SSI), except for the period during the Great Recession, where the
16
administrative values had more marked changes than self-reports. After 2000, the slopes are
quite similar for SSDI applications as well.
In general, self-reported values of applications and receipt of SSI are also lower than
administrative data, though the difference between the two are more modest than for SSDI,
especially after 2000. As mentioned above, prior to 2000, the HRS queried respondents about
SSDI and SSI in the same question, with the RAND-HRS separating responses where possible
later. Because we only accounted for known program status, and the SSI values are substantially
lower using that measure than one that accounts for uncertainty (not shown). After 2000, the
difference between self-reported and administrative values were relatively modest, fluctuating
between 2 and 2.5 percent in each year. The share of respondents who had ever applied for SSI
increased from 0.5 percent in 1996 to almost 8 percent by 2016 based on self-reports compared
with a change from 4.5 to nearly 10 percent based on administrative values.

17
Figure 2. SSDI and SSI Application and Receipt in HRS Survey Waves from 1996 through 2016
Notes: Limited to respondents born from 1936 through 1959 and part of the HRS, War Baby, and Early and Middle Boomer cohorts of the HRS. Values are
weighted to produce nationally representative estimates in the year, as described in the text.
Source: Authors’ calculations using the RAND-HRS and SSA data linkage.
18
The annual values in Figure 2 combine patterns over time based on secular patterns in
experience with federal disability programs, differences in patterns across HRS cohorts
(reflecting a range of factors including labor market conditions experienced by each cohort and
sufficient labor force participation to be insured for SSDI), as well as aging of cohorts in the
HRS as they are followed over time. We next disaggregate the data shown in Figure 2 to
highlight differences in self-reported and administrative values for each cohort in our analysis.
Figure 3 highlights the same four outcome measures, but the horizontal axis has been reoriented
from calendar time to the wave of the HRS interview relative to the first interview for each of
four cohorts. As shown in Table 1, the HRS cohort was first interviewed in 1992, the War Baby
cohort in 1998, the Early Baby Boomers in 2004 and the Late Baby Boomers in 2010. In each
case, that wave is “wave 1” in Figure 3; the HRS cohort therefore does not have data until wave
3 which occurred in 1996 when the DAF data began.
In Figure 3, the solid line for each cohort represents the self-reported value in the wave
relative to sample entry, while the dashed line of the same color represents the value from the
administrative data. The figure does not show that there are strong patterns by cohort across all
four measures, either comparing across cohorts or comparing self-reports to administrative
records. More recent cohorts tend to overstate their receipt of SSDI relative to administrative
records, aligning with the pattern shown in Figure 2 where self-reported receipt exceeds the
administrative record in the later years of our analysis period. Patterns are less clear for SSDI
application or the SSI measures. One pattern for SSI receipt is a product of our sample
definition: we include respondents through FRA but the SSI program after age 65 reflects old-
age benefits; this may explain the declining SSI receipt among self-reports in the last waves for
the cohorts that reach FRA. Those cohorts also may be misreporting SSI as OASI at those
points, though we did not explore that possibility.
Maestas et al. (2015) found increased SSDI participation during and following the Great
Recession of 2008; we would expect to see this primarily in 2010 given the HRS survey timing.
This corresponds to Wave 7 for the War Baby Cohort and Wave 4 of the Early Baby Boomers.
We do not see notable deviations from the previous trend in SSDI or SSI application or receipt at
that point for those cohorts, either in the self-reported or administrative data. By wave 7 of the
War Baby cohort, much of the sample had passed the earliest age of retirement at 62, so it may
be that the cohort claimed OASI early and did not meet the criteria for SSDI.

19
Figure 3. SSDI and SSI Application and Receipt for each HRS Cohort from Entry through FRA or 2016
Notes: Limited to respondents born from 1936 through 1959 and part of the HRS, War Baby, and Early and Middle Boomer cohorts of the HRS. Values are
weighted to produce nationally representative estimates in the year, as described in the text.
Source: Authors’ calculations using the RAND-HRS and SSA data linkage.

20
Age Profiles of SSDI and SSI Application and Receipt
Next, we examine reporting of SSDI and SSI applications and benefits by age. To do
this, we reoriented the data collected across many years, such that all respondents are “stacked”
by the same age (i.e., 51-52, 53-54, etc.),
6
regardless of the corresponding data wave. This
structure allows direct comparisons by age but does not consider compositional effects of cohorts
or time. These results are weighted using our IPW method described above but run by age
interval rather than by wave. We then apply the IPW to the wave weight available in the RAND-
HRS for the respondent at the relevant age. These estimated are therefore nationally
representative of the age group across all of the survey years.
Figure 4 displays the percentage of respondents who self-reported SSDI and SSI
application and/or receipt alongside corresponding percentages from SSA administrative records.
We show values at each age and interpret these values as a measure of wave-specific prevalence
of having applied to or receiving benefits. It is important to note that not all the HRS cohorts
have data at each of the ages; the values shown include all of the respondents at each age who
had data available. Table 1 highlights the years from which we identified respondents of a
particular age and cohort. For example, 51-to-54-year-olds are not included from the HRS
cohort because they were interviewed in 1992 and 1994, but our analysis begins in 1996. On the
other end of the age range, the Middle Boomers were last interviewed when ages 57-62. We
include the information we have available at each age, meaning that these analyses are not for
cohorts across the full age range we consider.
We report SSDI and SSI separately by program and also combined across programs. The
combined measure is designed to account for individuals who may know they have interacted
with a disability program administered by SSA but may incorrectly recall the program. If
misreporting reflects confusion of the program reported, we would expect this combined
measure to more closely align with SSA records than either of the individual program measures.
The top bar, in blue, corresponds to self-reports from the full HRS sample; this is the
value that users without access to the administrative linkage would report. The gray bar reflects
6
Note that the “age” we use is based on HRS survey wave and birth year, rather than actual age at interview, to
avoid issues with birth dates and HRS interviews that are not necessarily exactly two years apart. For example, a
respondent with a birth year of May 15, 1947, might have been 53 when interviewed by the HRS on May 31, 2000.
Yet when interviewed again on April 1, 2002, would only be 54. We would classify this respondent in the 53-54
age bin in 2000 and the 55-56 age bin in 2002.

21
the corresponding reports in the SSA administrative data, limited only to consenters. The blue
and gray bars mirror information reported by cohort and year earlier, simply transformed to
report by age instead. The middle orange bar represents self-reports from the HRS but is limited
to those who consented to SSA administrative linkage. The purpose of adding this bar is to
consider how different self-reports are among consenters relative to the full HRS sample
(comparing the blue and orange bars) and how different self-reports among consenters are from
their administrative linkage (comparing the orange and gray bars).
Figure 4 confirms again that HRS self-reports are generally lower than administrative
records for both the full sample and the subset who have consented to a data linkage. This is true
for SSDI receipt and SSI application and receipt (with the exception of SSI receipt at age 65 and
older).
7
In the case of SSDI applications, self-reports are higher than the administrative records
until age 60, after which the pattern switches. Despite finding that that respondents who consent
to the SSA data linkage differ on a number of demographic and health characteristics, the
aggregate patterns of reporting on application and receipt do not differ substantially between
consenters and the full HRS sample.
There is not a significant age gradient in the observed gaps between self-reports and
administrative reports; we expected we might see substantially more misreporting after age 62
when respondents could claim Social Security retirement benefits. There is modest evidence that
misreporting of benefits increases as respondents reach the earliest age of eligibility for Social
Security retirement benefits at age 62. For example, self-reports and administrative measures of
SSDI are much closer at ages 55-56 than at 63-64. Yet, we do not observe a similar pattern for
SSI, nor do we see that the combination of SSDI and SSI produces values that are substantially
closer across self-reports and administrative values. It is important to note that because the
composition of the sample is changing with age given the availability of data at older ages for
more recent cohorts, we cannot definitively conclude that self-reports at older ages reflect (or do
not reflect) confusion over the program from which benefits are being claimed.
7
The pattern at age 65-66 for SSI should be interpreted with caution; the SSI program after age 65 may be for old
age benefits rather than for disability. For consistency’s sake and to align with the DAF STW measure, we used this
value through full-retirement age, but there are reasons to think this comparison may reflect a different set of
considerations than at younger ages.

22
Figure 4. Comparisons of Percentage of SSDI and SSI Application and Receipt, by Age

23
Figure 4. Comparisons of Percentage of SSDI and SSI Application and Receipt, by Age (cont’d)
Notes: Limited to respondents born from 1936 through 1959 and part of the HRS, War Baby, and Early and Middle
Boomer cohorts of the HRS. Values are weighted to produce nationally representative estimates at each age, as
described in the text. SSDI or SSI refers to the total number of respondents who report either program; some
respondents report only one program and some report to both.
Source: Authors’ calculations using the RAND-HRS and SSA data linkage.
24
The Individual Accuracy of Self-Reported Responses About SSDI and SSI Application and
Receipt
Having described patterns of reporting in the aggregate—by wave, cohort, and age—we
now turn to describing the accuracy of individual self-reports. We focus on two age groups, 55
years old, the age at which there are likely to be the greatest number of respondents with data,
and 63, prior to FRA. For both SSDI and SSI, we categorize reporting into one of four groups.
Correct negative means that a respondent reports not having applied for or is receiving SSDI (or
SSI) and the corresponding administrative record concurs. Likewise, correct positive means a
concurrence in self-reports and administrative data for respondents who have applied or received
benefits. A false positive misreport indicates that a respondent indicates they have applied or are
receiving benefits whereas administrative records do not indicate application or receipt. Finally,
a false negative misreport is the opposite—respondents report no application or receipt and
administrative data does record an application or receipt. We report all data on misreports
without using sampling weights; we are interested in the likelihood of misreporting by groups of
respondents and therefore nationally representative estimates are not appropriate in this context.
Figure 5 displays the distribution of reports for SSDI and SSI applications, at age 55 and
63, by their accuracy. The blue segment of each bar correct negatives. Because a minority
interact with disability programs, this segment of the bar is the largest, representing 85 to 90
percent of all respondents. The orange segment of the bar represents correct positives; this
segment is far smaller than the blue bar simply because relatively few older adults receive
benefits. The gray and yellow segments of the bars show false positives and false negatives,
respectively. Together, these bars represent the share who misreport their benefits, which is
small relative to the full sample; 7-8 percent of HRS respondents misreport SSDI applications.

25
Figure 5. The Accuracy of Self-reported SSDI and SSI Applications at Ages 55 and 63
Notes: Limited to respondents born from 1936 through 1959 and part of the HRS, War Baby, and Early and Middle
Boomer cohorts of the HRS. Values are unweighted. “SSDI/SSI” refers to the total number of respondents who
report either program; some respondents report only one program and some report to both.
Source: Authors’ calculations using the RAND-HRS and SSA data linkage.
Another way to consider the magnitude of misreporting is to consider false reports as a
share of total reports within a given category. This allows for a much closer inspection of the
effect of misreporting on aggregate values. For example, consider SSDI applications at age 63
(Figure 5), where 18.6 percent of the total respondents with a self-report or administrative record
indicated an application. The share of false positives (3.9 percent) is close to the share of false
negatives (4.7 percent), yet false negatives represent a lower share of the total negatives than
false positives relative to total positives. This means that positive self-reports are more likely to
be wrong relative to the administrative record; 26.4 percent of positive self-reports were
incorrect (3.9 of 14.8 percent) compared to only 5.5 percent of negative self-reports (4.7 of 85.2
26
percent). Other than SSDI applications at age 55, the share of reports that is false negative is
larger than share that is false positive.
Figure 6 displays similar results for the receipt of benefits at ages 55 and 63, with similar
patterns. Overall, correct negatives are the largest share of reports, consistent with disability
program participation. While misreports are a small share of the total, they are much larger
when compared to total positive reports. Again, we see that for these outcomes, false negatives
are more common than false positives.
It is helpful to compare the distributions in Figures 5 and 6 to the total misreports in
Figure 4. In Figure 6, the percentage of receipt of a program is the sum of correct positives and
false negatives. For example, the percent of respondents receiving SSDI at age 55 from Figure 6
is 7.1 percent—5.1 percent (correct positives) plus 2.0 percent (false positives). The equivalent
value in Figure 4 is represented by the orange bar, self-report for those who consent to a linkage
and therefore have a corresponding administrative record from which we can assess
misreporting. In this case, the percent of 55-year-olds with an SSDI application is 6.4 percent.
Because the values in Figure 4 are weighted and those in Figures 5 and 6 are not, we expect these
values to be similar—as they are—but not necessarily identical.

27
Figure 6. The Accuracy of Self-reported SSDI and SSI Receipt at Ages 55 and 63
Notes: Limited to respondents born from 1936 through 1959 and part of the HRS, War Baby, and Early and Middle
Boomer cohorts of the HRS. Values are unweighted. “SSDI/SSI” refers to the total number of respondents who
report either program; some respondents report only one program and some report to both.
Source: Authors’ calculations using the RAND-HRS and SSA data linkage.
We sought to understand the characteristics of respondents who misreported, to assess
whether misreporting is concentrated in particular subgroups. In Tables 3a and 3b, we examine
selected differences in demographic and health characteristics for respondents who misreported
the receipt of benefits. We focus on receipt of benefits simply to avoid a vast number of
comparisons; results from a similar analysis for application are available upon request. In Table
3a, we compare differences between the false positive group relative to the correct positive
group. In Table 3b, we compare differences between the false negative group and correct
negative group.
These tables contain several simplifications to aid in interpretation. First, we limit to
characteristics in which we identified statistically significant differences between those who
28
report correctly versus those who misreport in at least one of the outcomes we considered. To
simplify the presentation further, we focus on groups of variables (e.g., race includes white,
Black and other where we tested the difference in the racial distribution of the groups). A check
in the box indicates that the mean or distribution of the variable category shown was statistically
different across the two groups. Appendix Tables B.3 and B.4 contain full results of these
comparisons.
Starting with Table 3a, we find that there are differences between those who misreported
that they were receiving benefits (false positives) relative to those who correctly reported they
were receiving benefits (correct positives). We do not observe consistent patterns in the
characteristics correlated with misreporting across program or age. For 55-year-olds,
misreporters of SSDI receipt differed from correct reporters by race, gender, marital status,
educational attainment of respondents. Those with false positive reports for SSDI at age 55 were
also more likely to report poorer health (with higher prevalence of high blood pressure and a
higher self-reported probability of having a work-limiting health condition in the next ten years)
and had worked for fewer years. At age 63, respondents with false positive for SSDI receipt
were twice as likely to be Hispanic, had an average of nearly one less year of education, had an
average of four less years of employment over their lifetimes, and scored higher on the CESD
mental health test.
We also observe demographic and health differences for false positive reports among 55-
year-olds relative to correct positives for SSI, but they are not the same characteristics as for
SSDI. SSI misreporters differ from correct reporters on race and ethnicity, as well as on average
income and assets. Notably, false positive reporters are more likely to have higher incomes and
assets (which might be expected, given the income and assets limits for SSI). There are also
health differences between false and correct positives; those with false positive reports tend to
have better health behaviors but report worse health. Those with false positive reports are less
likely to be smokers, report drinking fewer alcohol drinks per day, are less likely to report having
a psychological problem, have had more hospital stays in the last two years, and have higher out-
of-pocket medical expenditures. In general, the patterns of differences in misreporting SSI at age
63 reflect a different set of characteristics than at age 55.
Table 3b reveals that there are consistent differences between false negative and correct
negative reporters, across age and program. In fact, we find that there are statistically significant
29
differences across most individual characteristics. This pattern may not be particularly
surprising for two reasons. The first is sample size; correct negatives include all respondents that
have no program interaction with SSDI or SSI, which as shown in Figure 6, is the majority of the
sample. As such, sample sizes may be better powered to detect statistically significant
differences in characteristics. The second is the underlying truth in program participation. False
negative reporters are those actually receiving benefits and therefore meeting the financial and
health characteristics of the program. Because beneficiaries have significant health and
functional impairments and are generally out of the labor force, the differences in socioeconomic
and health characteristics are to be expected.

30
Table 3a. Differences in Demographic and Health Characteristics among Those Reporting
Benefit Receipt (check mark shows statistically significant differences between false positives
and correct positives
1
)
Age 55 receipt status
Age 63 receipt status
SSDI
SSI
SSDI
SSI
Demographic characteristics
Race
Ethnicity
Gender
Marital status
Socioeconomic characteristics and employment
Education (years)
Income
Assets
Working for pay
Self-reported probability of work-limiting
health condition in ten years
Total number of years worked
Health characteristics and behaviors
Has high blood pressure
Has lung disease
Has psychiatric problems
Current smoker
Number of alcoholic drinks per day
Body mass index (above 30 indicates
obesity)
CESD mental health score
2
Number of hospital stays in two years
Have visited the doctor in two years
Out of pocket medical expenditures
N (Correct positives)
437
156
492
95
N (False positives)
173
79
144
60
1
We used a t-test to compare the difference in means and a chi-square test to assess the difference in distributions.
When we tested the distribution, the test statistic is shown for the category heading.
2
Depressive symptoms measured by the Center for Epidemiological Studies Depression (CESD), an 8-point battery.
Notes: All values are taken at the ages 55 or 63, respectively, and all dollar values are inflated-adjusted to 2020
dollars.
Source: Authors’ calculations using the RAND-HRS and SSA data linkage.

31
Table 3b. Differences in Demographic and Health Characteristics among Those Not Reporting
Benefit Receipt (check mark shows statistically significant differences between false negatives
and correct negatives
1
)
Age 55 receipt status
Age 63 receipt status
SSDI
SSI
SSDI
SSI
Demographic characteristics
Race
Ethnicity
Gender
Marital status
Socioeconomic characteristics and
employment
Education (years)
Income
Assets
Currently working for pay
Probability living to 75/working to 65
Probability of work-limiting health condition in
next decade
Tenure from longest held job
Total years worked
Health characteristics and behavior
Self-reported health status
Health problems currently limit work
Doctor has ever diagnosed:
Blood pressure
Diabetes
Lung disease
Heart disease
Stroke
Psychiatric problems
Arthritis
Number of diagnosed health conditions
Memory problems
Back problems
Ever smoked/ Smoked now (%)
Number of alcoholic drinks per day
CESD mental health score
2
Number of ADL or IADL difficulties3
Hospital stays in previous two years (%)
Number of doctor visits in previous two years
Out of pocket medical expenditures
N (Correct negatives)
7,795
8,273
5,655
6,370
N (False negatives)
231
128
322
88
32
1
We used a t-test to compare the difference in means and a chi-square test to assess the difference in distributions.
When we tested the distribution, the test statistic is shown for the category heading.
2
Depressive symptoms measured by the Center for Epidemiological Studies Depression (CESD), an 8-point battery.
3
Activities of Daily Living (ADLs) and Instrumental Activities of Daily Living (IADLs) are marked 0-5 to
represent the number of ADLs/IADLs in which the respondent reports at least some difficulty.
Notes: All values are taken at the ages 55 or 63, respectively, and all dollar values are inflated-adjusted to 2020
dollars.
Source: Authors’ calculations using the RAND-HRS and SSA data linkage.
Comparing Aggregate Beneficiary Counts in the HRS Self-Reports and Administrative
Linkage to SSA Published Statistics
So far, we have considered the comparison within the HRS respondents of self-reports
and administrative values. We conclude by considering the number of SSDI and SSI
beneficiaries captured in the HRS relative to statistics published by SSA. To align as closely as
possible to published statistics, we made this comparison at two points in time, 2004 and 2010.
Those years reflect the addition of new cohorts to the HRS (Early Baby Boomers and Middle
Baby Boomers, respectively) so that the HRS sample is nationally representative of ages from 51
through FRA, which align with SSA statistics that span 50-FRA for SSDI and 50-64 for SSI. It
is important to note that while the statistics are similar, differences in the age composition of the
comparison as well as being measured at slightly different points in time means that our
comparison is valid within an order of magnitude, but we would not expect complete alignment.
Table 4 shows that: (1) self-reports are lower than administrative values in 2004 and
2010, consistent with our earlier findings, (2) administrative reports are lower than SSA
published statistics in both years, and (3) the magnitude of the discrepancy across sources is
smaller in 2010 than 2004. In 2010, the HRS linked to administrative records identified just
under 4.5 million SSDI beneficiaries, about 75 percent of the 5.8 million in SSA published
statistics. In the same year, the difference between the HRS administrative and published
statistics for SSI was about the same, with the 1.02 million SSI recipients identified based on
HRS administrative records reflecting about 78 percent of the 1.31 recipients in SSA published
statistics.

33
Table 4. Comparison of SSDI and SSI Beneficiaries in the HRS to SSA Published Statistics
SSA published statistic
1
HRS-SSA
administrative
HRS self-reports
SSDI beneficiaries
2004
4,247,536
3,603,152
3,103,867
2010
5,827,321
4,445,529
4,047,090
SSI beneficiaries
2004
1,350,000
994,285
838,508
2010
1,307,000
1,022,837
1,019,542
1
Published values for SSI beneficiaries reported by SSA in thousands.
Notes: SSA values include those ages 50 through FRA (SSDI) and 50 through 64 (SSI), while the HRS values
include those who are 51 through FRA to align with the selection criteria used in this manuscript. HRS values are
weighted to be nationally representative of the non-institutionalized population in the year based on HRS sampling
weights, as described in the text.
Source: SSA published statistics are from Table 4 of the SSDI Annual Statistical report
(https://www.ssa.gov/policy/docs/statcomps/di_asr/2019/sect01b.pdf) and the 2018 Annual Report of the SSI
program (available at https://www.ssa.gov/oact/ssir/SSI18/IV_B_Recipients.html#1020383). HRS values are
authors’ calculations using the RAND-HRS and SSA data linkage.
There are several possible reasons for the observed differences. First, the HRS sample in
these years is based on sampling weights that make the sample nationally representative of only
the non-institutionalized population. Starting in 2014, the HRS weights better account for
nursing home residence and no longer assign 0 weight to respondents living in an institution, but
that was not true in 2004 or 2010, nor the cohort selection processes for the samples in those
years. We could not find national statistics on the share of under-FRA beneficiaries residing in
institutions, we did find that 4.6 percent of the (unweighted) respondents receiving SSDI in 2010
had a zero survey weight (implying residing in an institution), and 5.2 percent of those receiving
SSI (not shown). Second, until 2016, the HRS only asked questions on SSDI and SSI to those
who reported a health-related work limitation. Those who were not asked the questions are
coded as not receiving benefits, yet we know from other work that about one-fifth of disability
beneficiaries in the CPS did not respond affirmatively to the survey question asking whether they
had a work-limiting health condition (Burkhauser et al. 2014). As a result, we expect that the
HRS self-reports will be lower than the administratively linked values. Those two factors alone
may explain the bulk of the observed gap between HRS reports and SSA published statistics. A
third explanation is that while the HRS is nationally representative on a range of characteristics,
it may not fully capture disability beneficiaries. Given that beneficiaries have significant health
limitations, it may not be surprising that they may be less likely to participate in a long survey
34
like the HRS and that the weighting procedure used by the survey may not account for all their
characteristics. Again though, we caution that we do not know the relative magnitude of these
three factors.
Discussion
We began this project by seeking a definitive answer to whether researchers should use
the HRS self-reported data or the administrative records. Our answer is perhaps an
unsatisfactory “it depends.” In many cases, the self-reported data may be accurate enough—if
receipt of SSI is simply a control variable, the difference between 2 percent and 2.5 percent may
not be important. Yet, if the research question involves the need for benefits status that aligns
with administrative records, or if the project intends to use other information about denied or
allowed applicants such as time to initial decision or reason for denial, the administrative records
are almost certainly better.
Our findings show that among the 15 percent or so of respondents with some information
indicating interactions with federal disability programs, about half of self-reported responses to
questions about having ever applied to or currently receiving SSDI or SSI in the HRS do not
align with the individual’s administrative record maintained by SSA. In general, we found that it
is more likely that respondents fail to report benefits they are receiving than reporting benefits
they are not receiving. On net, we found that the overall prevalence rates of SSDI and SSI
application and receipt when weighted to be nationally representative in the HRS are lower based
on self-reports than based on the administrative data. This is generally true across HRS
respondent ages and across cohorts in the HRS.
Despite level differences in the share of respondents reporting interactions with disability
programs, the patterns of new applications and new receipt across ages and waves in the self-
reported and administrative data look generally similar. In other words, the level differences that
we observe when respondents first enter the survey appear to remain over future waves. This
suggests that the introduction of early OASI benefits at age 62 likely does not exacerbate
misreporting, nor did we find strong evidence that respondents were reporting SSDI when they
meant SSI (the gap when looking at either SSDI or SSI looked about the same as when
considering each program separately).
35
We do not fully understand the causes of misreporting. In some instances, it may be a
mismatch between what is recorded in the administrative data and what is salient to an
individual. An applicant may not know that he or she was considered for SSDI when applying
for SSI or that the lack of a cash payment in the month does not mean beneficiary status has
ended. Yet, as we describe in detail in the appendix primer, most of the reasons we might expect
a mismatch between the data sources would result in an overstatement of self-reports relative to
administrative records. We did find that misreports are non-random and differ across race,
gender, income, employment history, and a number of health conditions and health behaviors.
We also found—as others have with older versions of the files—that consenting to the
administrative linkage is non-random. We attempted to account for this using a simple IPW
scheme that the HRS also uses for its other SSA linkages, though a more in-depth approach to
reweighting, such as exactly matching participants on certain characteristics, may be warranted
in other research contexts. More importantly though, researchers considering using the linked
data should be able to use our analysis to take stock of the effects on sample size. The richness
of the HRS questionnaire should not be understated, but for low-frequency events like disability
benefit receipt, a small sample size made smaller by a less-than-full consenting to the linkage
may make certain research studies intractable. Understanding the sample size loss may lead
some to accept the loss of precision in the self-reports in order to preserve record count.
Another reason that researchers may avoid the administrative records is a very high
barrier to entry. While the HRS has made strides in recent years to streamline and simplify the
process necessary to access the linked data, the documentation to understand and link the files to
the core survey remains complex and limited. Even with the addition of the DAF—which was
designed to support research on disability programs by linking information contained in other
files already accessible by HRS users—a detailed knowledge of SSA programs and program data
is required to work with the linked data. We have attempted to fill some of that gap with this
paper and the associated primer, but caution that the administrative records were not primarily
designed to support research and utmost caution is required to avoid misinterpretation of the
information they contain.
Because of the high barriers to entry, we suspect that self-reports will remain the
dominant source of information on disability benefit receipt using the HRS. Despite the
misalignment with the administrative records, there are several reasons that this may be
36
advantageous. First, the HRS is continually making improvements in the information it collects
from respondents. For example, in 2016, the HRS began asking all respondents—not only those
reporting a health-related work limitation—about their receipt of SSDI and SSI, recognizing that
a share of beneficiaries would not report such limitations. Second, the HRS collects a large
battery of information about disability onset that goes beyond program participation. For
example, the survey asks respondents about the nature of their limitation, the timing of new
onset, and about their own and their employer’s responses to new health conditions. To the
extent that self-reported information about program participation aligns with the respondent’s
recall about the other disability measures, self-reported data across the board may be preferable
to combining information from other sources.
A third and final benefit of the self-reported information is that the RAND-HRS files take
an incredibly complex question sequence with variability over the two decades of HRS data
collection to produce a streamlined, quickly accessible set of measures related to participation in
SSDI and SSI. The herculean effort that went into producing cross-wave consistent measures of
program participation should not be understated, and we suspect that many studies of those
measures would not have been conducted if researchers themselves had to develop those
measures independently using the core HRS files. The HRS has significantly advanced the
knowledge base related to older workers with new disabling conditions because of its rich,
longitudinal data collection and care to preserve measures as much as possible over time to
produce cross-wave consistency. The RAND-HRS files have built upon that notable data
collection to make the information widely accessible by the research community. Without both
components, we suspect that our understanding of disabilities among older workers would be
substantially less robust.
Conclusion
In this paper, we sought to investigate differences in consenting to and reporting of SSI
and SSDI application and receipt between self-reported and linked SSA administrative data in
the HRS. We find that aggregate self-reported percentages of application and receipt of SSDI
and SSI are lower than those reported in HRS-SSA administrative data at nearly all ages, but
incidence rates are similar. Moreover, there are cohort differences in the rates of application and
receipt of self-reports and administrative data on application and receipt of SSDI or SSI but no
37
consistent pattern in the difference between the two across the cohorts. Individual misreporting
represents a minority of cases but is still common among those, and false negatives (i.e.,
reporting no application or receipt despite administrative records indicating otherwise) tend to be
higher than false positives, especially at older ages. Characteristics among respondents who
provide false self-reports as compared to their linked administrative data differ from those whose
self-reports are concordant with administrative records. Those differences depend on the
program and age of the respondents, but include race, income, assets, education, health
conditions, and health behaviors.
Taken together, we find that both data sources can be useful for research pertaining to SSI
and/or SSDI applicants or beneficiaries, depending on the research question at hand. Using HRS
self-reported data is likely to result in an underestimate of program application and receipt relative
to HRS-SSA data and descriptions of applicants or recipients’ demographics, employment,
income, and health may differ. As such, care should be taken in interpreting applicant or
beneficiary characteristics when using self-reports. Still, use of linked data may not be feasible
for some research purposes. In cases where a linkage may not be practical, the use of self-
responses can still be informative in a number of research applications. These can include, and
are not limited to, longitudinal analysis of employment or health characteristics in relation to SSA
programs or the use of receipt or beneficiary status as covariates or controls in analysis.

38
References
Bee, Adam and Joshua Mitchell. 2017. “Do Older Americans Have More Income Than We
Think?” SESHD Working Paper no. 2017-39. Washington, DC: U.S. Census Bureau.
Available at: https://www.census.gov/content/dam/Census/library/working-
papers/2017/demo/SEHSD-WP2017-39.pdf
Burkhauser, Richard V., T. Lynn Fisher, Andrew J. Houtenville, and Jennifer R. Tennant. 2014.
“Is the 2010 Affordable Care Act Minimum Standard to Identify Disability in All
National Datasets Good Enough for Policy Purposes?” Journal of Economic and Social
Measurement 4: 217-245.
Chen, Anqi, Alicia H. Munnell, and Geoffrey T. Sanzenbacher. 2018. “How Much Income Do
Retirees Actually Have? Evaluating the Evidence from Five National Datasets.” Working
Paper 2018-14. Chestnut Hill, MA: Center for Retirement Research at Boston College.
Davies, Paul S. and T. Lynn Fisher. 2009. “Measurement Issues Associated with Using Survey
Data Matched with Administrative Data from the Social Security Administration.” Social
Security Bulletin 69(2): 1-12.
Health and Retirement Study (HRS). March 2021. “Social Security Weights (2004-2016).” Ann
Arbor, MI: University of Michigan. Available at:
https://hrs.isr.umich.edu/sites/default/files/restricted_data_docs/SSWgts_JP_DD%20v2.p
df
Health and Retirement Study (HRS). 2021. “Cross-Wave Social Security Consent File.”
Undated. Ann Arbor, MI: University of Michigan. Available at:
http://hrsonline.isr.umich.edu/modules/meta/xyear/consents/codebook/ConsentSSA.txt
Hyunh, Minh, Kalman Rupp, and James Sears. 2002. “The Assessment of Survey of Income and
Program Participation Benefit Data Using Longitudinal Administrative Records.” Survey
of Income and Program Participation Report No. 238. Washington, DC: U.S. Census
Bureau.
Koenig, Melissa. 2003. “An Assessment of the Current Population Survey and the Survey of
Income and Program Participation Using Social Security Administrative Data.” Paris,
France: OECD. Available at: http://www.oecd.org/std/36232612.pdf
Maestas, N., K. J. Mullen, and A. Strand. 2015. “Disability Insurance and the Great
Recession.” American Economic Review 105(5): 177-182.
Meyer, Bruce D. and Nikolas Mittag. 2019. “Using Linked Survey and Administrative Data to
Better Measure Income: Implications for Poverty, Program Effectiveness, and Holes in
the Safety Net.” American Economic Journal: Applied Economics 11(2): 176-204.

39
Meyer, Bruce D., Wallace K. C. Mok, and James X. Sullivan. 2015. “Household Surveys in
Crisis.” Journal of Economic Perspectives 29(4): 199-226.
Phillips, John. 2003/2004. “The RAND HRS Data File: A User-Friendly Version of the Health
and Retirement Study.” Social Security Bulletin 65(2): 97-98.
Schimmel Hyde, Jody, Sarah Croake, Alex Bryce and Matthew Messel. 2018. “Developing
Income-Related Statistics on Federal Disability Beneficiaries Using Nationally
Representative Survey Data.” Mathematica DRC Working Paper 18-05. Washington,
DC: Mathematica.
Schimmel Hyde, Jody and David C. Stapleton. 2017. “Using the Health and Retirement Study
for Disability Policy Research: A Review.” Forum for Health Economics and Policy
20(2).
Singer, Eleanor. 2006. “Introduction: Nonresponse Bias in Household Surveys.” Public Opinion
Quarterly 70(5): 637-645.
Smith, James P. 2003. “Consequences and Predictors of New Health Events.” Working Paper
No. 10063. Cambridge, MA: National Bureau of Economic Research.
40
Appendix A. A Primer for Using Information in the Health and Retirement Study to
Measure Experiences with Federal Disability Programs
The Health and Retirement Study (HRS) offers an opportunity to measure experiences
with disability program interactions using individuals’ self-reports as well as administrative data
collected by the Social Security Administration (SSA). Because of the cross-wave consistent
measures contained in the RAND-HRS, working with the self-reported data is relatively
straightforward and these variables are commonly used in disability-related research using the
HRS. The administrative data made available by SSA, however, may be more appropriate in
some cases—for example, when looking at the reason for benefit allowance, the timing of benefit
cessation, or when accurate benefit information is critical. Working with the administrative data
poses additional hurdles, which may in part explain why the linked resource has been
underutilized (Schimmel Hyde and Stapleton, 2017). Among these, understanding how to work
with the administrative data, which are not designed for research and are not well-documented,
may be most critical.
In this document, we offer a primer for developing measures of application to and receipt of
Social Security Disability Insurance (SSDI) and Supplemental Security Income (SSI) based on
the administrative data. We describe our approach to identifying (1) whether HRS respondents
have ever applied for SSDI or SSI by the time of each HRS interview, and (2) whether they are
receiving SSDI or SSI as of each interview. We do this using the SSA administrative linkage as
well we the RAND version of the HRS. Researchers who are interested in using data from these
sources may find this document a starting point for their own research, though we recognize that
the decisions we made for our work might not apply in all circumstances. Each source of
information has relative strengths and weaknesses; we hope these will become apparent in what
follows.
Data Sources
We use four main sources of information in this document to measure application for and
receipt of SSDI and SSI benefits:

41
1. The RAND-HRS, which contains cross-wave consistent information about SSI and SSDI
benefits, derived from respondent self-reports in the HRS. For our analysis, we used the
version of the file that contained data through 2018.
2. Form 831 Respondent Records. This is an SSA administrative file available with
permission to HRS users that contains information on most initial applications for SSDI
and SSI from 1988 onward. As we describe below, the file is limited to applications that
received a medical review. The version of the file we worked with to develop this primer
contained applications through 2016.
3. Disability Analysis File (DAF). The DAF is an SSA file that combines data from
multiple administrative sources to produce monthly information about the receipt of
SSDI and SSI benefits starting in 1996. The version of the file we worked with to
develop this primer contained information through 2018.
8
4. The HRS-SSA Permissions Consent History. This file provides information in each
HRS wave whether a respondent to the HRS consented to having their information linked
to SSA records and whether a match with the data was found. This file is critical for
knowing which respondents might have administrative records available.
Additionally, users who solely want to work with the administrative data may want to consult
the HRS-SSA Weights File, which provides weights that may be used to account for
nonresponse due to not consenting in order to construct a nationally representative sample.
Depending on the specific analysis, researchers may want to use these weights or construct their
own weights using a similar methodology.
8
Instead of this file, a researcher could use the Cross-Year Benefits File (CYBF) and the SSI Respondent File that
are available to HRS users. In theory, those files allow you to construct monthly measures of benefit receipt. We
encountered significant difficulty in using the CYBF to identify months in which benefits were paid for SSDI versus
Old Age and Survivors Insurance (OASI) benefits, which is a critical distinction between early and full retirement
age. We document some of the challenges we encountered in working with those files in what follows.

42
HRS-SSA Permissions and the Implications for Sample Selection
A subset of respondents in the HRS have information available in each of the
administrative records. Before beginning to work with the linked administrative records, it is
critical to understand the availability of data across HRS respondents and time. Missing
information in a particular linked file could be due to one of three reasons: (1) not having
interactions with federal disability programs, (2) not consenting to have data linked to the SSA
files, or (3) consenting to the linkage, but not providing data that allows for a successful match.
Thus, it is critical to understand who gave permission in order to know whether their absence
from a given administrative record reflects no program interaction or simply not having available
data.
The process the HRS has used to ask its respondents to consent to having their data
linked has changed over time. Before 2006, respondents provided consent through the survey
year. In those years, if a respondent did not reconsent in a later year, data would only be
available through the last year consent was given. Starting in 2006, the HRS instituted a
prospective consent process that allowed data linkages into the future. These permissions are
collected and updated as needed during face-to-face interviews that the HRS conducts
periodically with respondents.
9
The duration of prospective permissions varies depending on the
year the consent was collected and whether the consent was for earnings or benefits.
10
The HRS documentation on permissions consent history provides additional information
about the years in which respondents provided permission and the share of consenting records
for whom matched earnings and benefits data is available.
11
Much of that documentation is
limited to those with access to the restricted data, but publicly available documents contain a
high-level overview that may be helpful before beginning work.
Based on correspondence with HRS staff, we learned that the DAF and 831 file were
only available for HRS respondents who consented to the linkage in 2006 and later. As such, we
9
About half of the HRS sample has a face-to-face interview in each wave. This means as a new cohort ages into the
sample, it takes two waves for most of the sample to have had the opportunity to consent to the SSA linkage.
10
Additionally, certain SSA files are only available if permission was obtained in 2006 and later; this applies to both
the 831 and DAF that we used for our analysis. For this reason, we constructed our own consent weights that
accounted for consent offered in 2006 or later, rather than the wave-specific weights provided by the HRS.
11
Based on correspondence with HRS staff, the process SSA uses to match each administrative file may vary
slightly and thus, there is not a consistent measure of whether the consenting record was matched. The consent file
provided by the HRS contains a “match” flag for whether the record matched to the MBR. Because our analysis did
not use that file, we did not use the match variable. Thus, the denominator of people who consented to the match is
likely a slight overestimate relative to the number who had data available to complete the match.
43
use the consent file to determine the most recent consent year and limited our analysis to 2006
and later, reweighting following the procedure the HRS uses to reweight the SSA-matched
sample to be nationally representative. Depending on the data files and waves of analysis, users
may be able to follow a similar process.
Because missing records in the administrative file may be due to several sources, in what
follows, we only define the affirmative value of each indicator. In other words, we define only
whether the administrative data indicates that the person applied for or received benefits. We do
not specify the lack of application or receipt. Users may do this differently, depending on how
they want to include non-consenters in their analysis. Some may choose to set any HRS
respondents to ‘0’ who are not an applicant/beneficiary in the administrative records, while
others may want to distinguish the reason for missing information (e.g., limiting to consenters
but who were not in the administrative data).
DI and SSI Benefit Receipt
Though applications predate benefit receipt chronologically, we discuss our approach to
constructing benefit receipt first. We do this because as we will show, there are reasons to think
that applications may be undercounted for HRS respondents who receive benefits in the early
years of the survey. As such, we use our measure of receipt to impute applications in some
instances.
Measuring SSDI and SSI Benefit Receipt Using the RAND-HRS
To identify beneficiaries in each wave, we use information from the RAND-HRS
RwDSTAT variable. The RwDSTAT variable indicates at each wave whether the person reports
having a pending application for benefits or is receiving them, separately by program. We define
two versions of SSI and SSDI beneficiary measures. The first definition is simply based on
affirmative self-reports of “yes, I receive benefits from SSI” or “yes, I receive benefits from
SSDI.” This can include concurrent benefit receipt, where respondents report both SSDI and SSI
receipt. These are defined directly from the information in the RAND-HRS, where the
categories capture combinations of benefit receipt and pending applications across SSDI and
SSI:

44
RwSSIBENSLF1=1 if RwDSTAT=2, 12, or 22
RwDIBENSLF1=1 if RwDSTAT=20, 21, or 22
The second definition accounts for the fact that respondents sometimes indicate that they
know they are receiving benefits from SSA but are not sure from which program the benefits are
being paid. This category is especially important before Wave 5, when the HRS did not
distinguish benefits from the particular program. When possible, the HRS attempted to collect
updated information from respondents after the survey changed, but that was not always
possible. As such, the share of respondents with unknown benefit status is much higher through
2000 than it is in later waves. The second definition expands upon the analogous first definition
by adding in another category that indicates benefit receipt from an unknown program:
RwSSIBENSLF2=1 if RwDSTAT=2, 12, 22, or 200
RwDIBENSLF2=1 if RwDSTAT=20, 21, 22, or 200
Measuring SSDI and SSI Receipt Using the SSA Administrative Linkage
We derive the receipt of SSDI and SSI benefits using the DAF, first linked to the HRS in
early 2021. The DAF draws information from nearly one dozen SSA administrative datasets and
provides information on SSDI and SSI receipt in a single file for all beneficiaries who have
received benefits since 1996. The timing of the DAF means that the first two waves of the HRS
do not have comparable administrative records.
12
Unlike other administrative sources, the DAF
is designed to support research on beneficiaries and thus is relatively easier to work with than
other administrative files on beneficiaries linked to the HRS.
We identify the receipt of benefits using the “STW” measure in DAF, which is a
constructed measure designed to indicate whether beneficiaries did not receive benefits in a
month because they were in suspense or termination status for work. Because the STW indicator
identifies suspense and termination for various reasons, the remaining category indicates
beneficiaries who were in current payment status in the month.
13
In general, current payment
12
The DAF contains data back to 1994 for beneficiaries who received benefits from 1996 onward but does not
contain complete information on all beneficiaries in 1994 or 1995.
13
The DAF variables LAFyymm and PSTAyymm can also be used to determine current payment status, but an error
in the version of the file we accessed meant that PSTA was excluded from the file. Users should consult future

45
status means that the beneficiary received a cash payment in the month, though STW can be
updated retroactively.
14
RwDIBENADM=1 if STWDIyymm=0 in the months of the HRS interview
15
RwSSIBENADM=1 if STWSSIyymm=0 and PAYSyymm>0 in the months of the HRS
interview
For SSI beneficiaries, we add a criterion beyond the STW measure for purposes of
comparing to the self-report. Because program rules allow SSI recipients to be in current
payment status but not receive a cash payment in the month (if their earnings or deemed income
are too high), we also restrict SSI beneficiaries to those who received a positive payment in the
interview month(s) (PAYS>0). We think the receipt of a cash payment may be most relevant to
an HRS respondent when they report the receipt of benefits in the survey. Depending on the
context of one’s research, this additional restriction may not be necessary.
As an alternative to using the DAF, some users might want to measure benefit receipt
using other administrative records linked to the HRS. For SSDI, researchers may consider the
Respondent Cross-Year Benefit File (CYBF), which is a combination of SSA’s Master
Beneficiary Record (MBR) and the Payment History Update System (PHUS). The file contains
information on receipt SSDI and Old Age and Survivors’ Insurance (OASI), and it is important
to identify the reason that benefits were paid. There are several measures that may be critical to
users, though it is important to understand the caveats of each.
• DOEITOB and DOECTOB indicate the type of benefit, keyed to the earliest and most
recent benefit spell, respectively. Using these measures, it is not possible to know if there
were intervening benefit spells or the dates/benefits received on those spells. This could
documentation about the DAF linked to the HRS to identify whether these values may offer additional information
beneficial to their research question.
14
It is possible that an HRS respondent might report in an interview that received benefits, but the DAF record
indicates they were in suspense status. Suspense and termination is relatively uncommon in the years just before full
retirement age, so this is likely to not be a common issue among HRS respondents.
15
Because HRS interviews can span more than one month and because we do not know precisely when benefits
status is reported by beneficiaries during that time, we looked for benefits in the interview beginning and end
months. Because few beneficiaries terminate from benefits, this is unlikely to substantially change the count of
beneficiaries but errs on the side of counting respondents as beneficiaries if their status changes over that time.
46
be especially important as individuals move from SSDI to OASI, and as such, we did not
consider these variables reliable for our purposes.
• TOC indicates the Type of Claim and is taken directly from the MBR. Up through May
2009, this value was overwritten with the most recent data. We were not able to identify
a variable in the linked file that identified the date that aligns to TOC. After May 2009,
multiple occurrences of TOC are recorded with corresponding TOCSTART dates (there
were 5 such occurrences in the version of the file we worked with). While we tried to
construct a series using the TOC values available, we were not able to do so in a way that
we considered reliable enough for our purposes.
For SSI, researchers may consider the Supplemental Security Income File, which is a
combination of SSA’s Supplemental Security Record (SSR) and its SSI Longitudinal File. The
SSI file contains monthly information back to 1974, when the SSI program started. Like
working with the CYBF, it is important to identify whether SSI is being provided on the basis of
disability or old age, or simply limiting SSI for disability to those under age 65. This can be
done using the MFT and/or TOA variables in the file.
The SSI file is stored with one record per year of benefits, with a summary file indicating
SSI spells. Beneficiaries can have multiple spells of SSI, either because they go on and off
benefits, the basis for receiving benefits changes, or simply because their record is so long than
SSA starts a new one (this has become less common as computing power has increased). It is
important to link data from multiple years to get a complete picture of SSI benefits history. Yet,
in the version of the linked file we worked with, we only found one record establishment date for
each respondent in the file, which is not what we would expect given the likelihood of multiple
SSI spells. As such, we suggest that users exercise caution when working with this file and
consult the HRS with any questions about its contents.
SSDI and SSI Applications
Measuring SSDI and SSI Application Using the RAND-HRS
We used the disability spell data in the RAND-HRS to identify whether respondents had
applied for benefits; the RwDSTAT variable indicates applications pending at the time of
interview but may miss applications that are adjudicated between HRS survey waves. At each

47
interview, we compared the interview date (RwIWEND)
16
to the RADAPPx (application date for
spell X) variables from RAND.
17
We looked for any spells that preceded the HRS interview date
and identified if respondents reported applying to SSDI, SSI, both, or if they were unsure which
program they applied for. Because we were only interested in having ever applied by a given
HRS wave, we did not construct measures for multiple applications, though it is possible to do so
with the information provided.
If any RADAPPx variable is before RwIWEND, we define a wave-specific measure of
which program the respondent reports applying for. We create two versions based on a narrow
and a broad definition, like what we did for benefit receipt to account for the uncertainty of the
program to which the respondent reports applying. The narrow definition version includes
applications in which the respondent indicated the program to which they applied. In addition,
this version accounts for respondents who report receiving benefits, but for whom application
data was not reported. The broad version builds off the narrow but incorporates uncertain
responses about the program from which benefits were sought.
RwSSIAPPSLF1=1 if RADTYPE=2 for any RADAPPx < RwIWEND or
RwSSIBENSLF1=1 for current wave or any earlier wave
RwSSIAPPSLF2=1 RwSSIAPPSLF1=1 or if RADTYPE= 3, 12, 13, 21, 23
18
for any
RADAPPx < RwIWEND
RwDIAPPSLF1=1 if RADTYPE=1 for any RADAPPx < RwIWEND or
RwDIBENSLF1=1 for current wave or any earlier wave
16
Note that some HRS interviews span longer than a day, so there is a beginning and end date recorded. By taking
the end date, we account for any applications that might have started during the interview “period,” though we don’t
know when in the period the disability questions would have been asked. In most cases, this will not lead to
differences in information collected from beneficiaries.
17
The majority of respondents who report having applied for SSDI/SSI report 1 or 2 applications. In the RAND-
HRS 2016 longitudinal file, 7,175 respondents reported at least one application. Of those, 5,017 reported only one
application and 1,604 reported two applications.
18
The category 3 indicates that the respondent reported applying for both SSDI and SSI, but also that they don’t
know to which program they applied. Nearly 40 percent of respondents are in this category. The categories of 12,
13, 21, and 23 are far less common, but indicate changes in responses over time; for example, a respondent initially
reports in one wave that they applied for SSDI, but later says they applied for SSI.

48
RwDIAPPSLF2=1 if RwDIAPPSLF1=1 or if RADTYPE= 3, 12, 13, 21, 23 for any
RADAPPx < RwIWEND)
As we mentioned at the start of the receipt section, we include as applicants those
respondents who reported (with certainty) that they were receiving benefits from a given
program. We believe it is possible based on the HRS sequence that a person receiving benefits
could accurately report their benefits status but not provide complete information on their
applications. This might be especially true for those who began receiving benefits well before
they joined the HRS sample at age 51 or older.
Measuring SSDI and SSI Applications Using the SSA Administrative Linkage
Administrative information about application for SSDI and SSI benefits linked to the
HRS comes from the Form 831 file, which is the system that SSA uses to record the outcome of
initial applications that receive a full medical review. The 831 file are structured with one row
per application, separated by SSDI and SSI. For purposes of determining application status as of
each HRS interview wave, we first identify application dates for each program:
SSIAPPDT=Combine FLD_Y, FLD_M and DAY=15
19
if RID=16
DIAPPDT=FLD_Y, FLD_MY, and DAY=15 if RID=2
With those defined, we then construct one-row-per-respondent record of applications
using HHIDPN that incorporates all the SSI and SSDI application dates, so we can identify any
applications filed before the HRS interview date:
RwSSIAPPADM=1 if (any SSIAPPDTx < RIWEND) or RwSSIBENADM=1 for
current wave or any earlier wave
RwDIAPPADM=1 if (any SSDIAPPDTx < RIWEND) or RwDIBENADM=1 for current
wave or any earlier wave
19
To reduce disclosure risk, the files do not include the exact date of application. For simplicity, we assume the
15th of the month for purposes of constructing a single application date.

49
Like self-reports, we augment application data from the 831 file to incorporate
beneficiary status and assume that if the administrative record identified the respondent as a
beneficiary, they must have applied prior to that time. This would be true if the respondent
applied for benefits prior to 1988, when the 831 file began.
It is important to understand the information that is—and is not—contained in the 831
file and implications for how the 831 records might relate to self-reports. The 831 file includes
only the outcomes of applications that received a full medical review, which likely do not
capture the full range of applications that respondents might report. Form 831 records do not
include:
• Applications that have not yet received an initial determination.
• Received a “technical denial.” Technical denials occur when SSA determines that the
applicant did not meet the financial eligibility criteria for benefits before considering
their medical conditions. In the case of SSDI, this would mean not having sufficient
quarters of coverage to be SSDI-insured. For SSI, this might mean income or assets that
are too high. About one-third of applications receive a technical denial. In these
instances, HRS respondents might report having applied for benefits, but there would be
no record in the 831 file.
• Information about applications that are initially denied but subsequently appealed. For
purposes of identifying whether a respondent has ever applied for benefits, this is not a
problem, because the initial application is in the 831 file. As such, an HRS respondent
could accurately report a pending claim that would not be in the 831 file. About half of
applications are rejected at the initial or reconsideration levels, with many ultimately
receiving an award. Using the 831 file, it is impossible to know which applications have
been appealed.
There are also reasons why applicants might not know that they have an application that
is recorded in the 831 file. For example, an individual who applies for SSI is automatically
considered by SSA for SSDI as well, by checking the quarters of coverage the applicant has.
Applicants to SSDI will be considered for SSI if they report having low income or assets. Yet,
50
respondents may not fully understand the distinction across programs and thus may not know
that they had an application to a program other than the one from which they initially applied.
There is a measure in the 831 file, CCF, that indicates that a concurrent application was
filed, meaning that the applicant initially sought both SSDI and SSI benefits. In many cases,
applications marked with CCF in the 831 file have an application to the other program with the
same filing date, meaning that the applicant met the criteria for both programs. There are other
applications, however, in which the application is flagged as concurrent, but there is only one
application from that date (e.g., a SSDI application is in the 831 file without an analogous SSI
application). In those cases, the applicant applied for benefits from both programs, but for one of
the programs, the application was denied before receiving a medical review (technical denial).
Thus, using CCF would allow researchers to fill in additional information about some
applications. Still missing are applications to only one program that were technically denied, as
well as concurrent applications that were technically denied to both programs. Because we know
that even with CCF, we do not know the full account of technical denials, we do not use CCF
records in our analysis.
51
Appendix B. Supplementary Tables
Appendix Table B.1. Interview and Consent Status of HRS Respondents by Cohort and Wave (Unweighted)
1992
1994
1996
1998
2000
2002
2004
2006
2008
2010
2014
2016
HRS (born 1936-1941)
Interviewed
5,604
5,045
4,788
4,578
4,336
3,207
1,981
723
0
0
0
0
Never consented
670
508
439
394
346
248
139
40
0
0
0
0
Consented pre-2006
2,186
1,902
1,730
1,565
1,389
950
550
170
0
0
0
0
Consented 2006 or later
2,748
2,635
2,619
2,619
2,601
2,009
1,292
513
0
0
0
0
Not interviewed, not dead
0
487
645
760
877
750
513
269
0
0
0
0
Reached FRA
0
0
0
0
0
1,213
2,796
4,435
5,604
5,604
5,604
5,604
Dead (before FRA)
0
72
171
266
391
434
314
177
0
0
0
0
War Baby (born 1942-1947)
Interviewed
0
0
0
3,090
2,834
2,752
2,634
2,526
2,141
1,290
569
0
Never consented
0
0
0
473
358
313
250
232
189
133
61
0
Consented pre-2006
0
0
0
656
571
528
472
381
285
146
55
0
Consented 2006 or later
0
0
0
1,961
1,905
1,911
1,912
1,913
1,667
1,011
453
0
Not interviewed, not dead
0
0
0
0
227
257
337
379
395
264
139
0
Reached FRA
0
0
0
0
0
0
0
0
322
1,365
2,290
3,090
Dead (before FRA)
0
0
0
0
29
81
119
185
232
171
92
0
Early Baby Boomers (born 1948-1953)
Interviewed
0
0
0
0
0
0
3,369
3,019
2,892
2,803
2,683
2,394
Never consented
0
0
0
0
0
0
578
419
372
346
327
290
Consented pre-2006
0
0
0
0
0
0
449
349
265
225
190
155
Consented 2006 or later
0
0
0
0
0
0
2,342
2,251
2,255
2,232
2,166
1,949
Not interviewed, not dead
0
0
0
0
0
0
0
311
388
416
487
538
Reached FRA
0
0
0
0
0
0
0
0
0
0
0
162
Dead (before FRA)
0
0
0
0
0
0
0
39
89
150
199
275
Middle Baby Boomers (born 1954-1959)
Interviewed
0
0
0
0
0
0
0
0
0
4,782
4,394
4,125
Never consented
0
0
0
0
0
0
0
0
0
1,019
834
761
Consented pre-2006
0
0
0
0
0
0
0
0
0
59
44
45
Consented 2006 or later
0
0
0
0
0
0
0
0
0
3,703
3,515
3,318
Not interviewed, not dead
0
0
0
0
0
0
0
0
0
0
333
537
Reached FRA
0
0
0
0
0
0
0
0
0
0
0
0
Dead (before FRA)
0
0
0
0
0
0
0
0
0
0
55
120
Source: Authors’ calculations using the RAND-HRS and SSA data linkage.

52
Appendix Table B.2. Comparison of Characteristics in the Full HRS Sample and Consenter
Sample (Unweighted)
Full HRS
sample
Consenter
sample
p-value
1
Demographic Characteristics
Race (%)
White
74.0
76.2
0.0002***
Black
18.3
16.4
Other
7.7
7.4
Ethnicity (%)
Hispanic
12.1
11.7
0.4569
Non-Hispanic
87.9
88.3
Gender (%)
Male
41.0
38.4
<.0001***
Female
59.0
61.6
Marital Status (%)
Married
87.6
87.3
0.1655
Divorced
6.5
7.1
Never married
5.9
5.6
Education (years completed)
12.5
12.7
<.0001***
Socioeconomic characteristics and employment
Respondent income ($)
24,352
25,490
0.0445*
Household income ($)
70,411
71,186
0.6509
Total household assets ($)
278,602
277,852
0.9315
Labor Force Status
In labor force
68.0
71.9
<.0001***
Retired
17.8
15.6
Disabled
5.3
4.3
Not in labor force
8.9
8.2
Years of tenure at current job
12.0
11.7
0.1058
Years at longest job
15.7
15.4
0.0277
Total years worked
26.9
26.8
0.4943
Health Characteristics
Self-reported health (%)
Excellent
16.8
18.1
<.0001***
Very good
30.6
32.1
Good
28.9
28.5
Fair
16.8
15.8
Poor
6.9
5.5
Health problems limit work
24.1
21.5
<.0001***
Doctor has ever diagnosed (%):
High blood pressure
37.4
35.7
0.0066***
Diabetes
12.5
10.6
<.0001***
Cancer
6.1
5.6
0.0859
Lung disease
5.7
4.5
<.0001***
Heart disease
11.1
9.5
<.0001***
Stroke
3.2
2.5
0.0006***
Psychological problem
12.1
12.4
0.383
Arthritis
37.3
36.3
0.138
53
Total number of health conditions reported
1.3
1.2
<.0001***
Body mass index (above 30 indicates obesity)
28.2
28.4
0.0066***
CESD mental health score
2
1.5
1.4
0.4454
Number of ADL difficulties
3
0.213
0.179
0.0002***
Number of IADL difficulties
4
0.17
0.138
<.0001***
Hospital stay in previous two years (%)
18.4
17.0
0.005*
Any doctor visit in previous two years (%)
89.9
90.4
0.2045
Number of doctor visits in previous two years
8.3
8.0
0.0912
Out-of-pocket medical expenditures ($)
2,248
2,165
0.3467
Self-reported probability of (%):
Living to age 75
64.3
65.6
0.0023**
Working full-time after age 62
46.3
46.3
0.976
Working full-time after age 65
28.9
29.1
0.7075
Work-limiting health problem in next decade
38.8
38.3
0.4421
Health Behaviors
Ever smoked (%)
59.2
57.4
0.0051
Smokes now (%)
23.2
21.8
0.0068**
Ever drank alcohol (%)
57.9
60.2
0.0002***
Number of days/week of drinks with alcohol
1.1
1.2
0.0199**
Number of drinks of alcohol per day
0.9
1.0
0.3868
1
We used a t-test to compare the difference in means and a chi-square test to assess the difference in distributions.
When we tested the distribution, the test statistic is shown for the category heading.
2
Center for Epidemiological Studies Depression (CESD) is an 8-point battery measure depressive symptoms.
3
Activities of Daily Living (ADLs) marked 0-5 to represent the number of ADLs in which the respondent reports at
least some difficulty.
4
Instrumental Activities of Daily Living (IADLs) are marked 0-5 to represent the number of IADLs in which the
respondent reports at least some difficulty.
Notes: ***p<0.001; **p<0.01; *p<0.05. All values are taken at baseline (i.e., when the respondent was first
observed in our sample), and all dollar values are inflated-adjusted to 2020 dollars.
Source: Authors’ calculations using the RAND-HRS and SSA data linkage.

54
Appendix Table B.3. Comparison of Characteristics of Respondents Who Correctly Report and Misreport Receipt of SSDI Benefits at
Age 63-64 (Linked Respondents, Unweighted)
Correct
Positive
False
Positive
p-value
1
Correct
Negative
False
Negative
p-value
1
Demographic characteristics
Race (%)
White
72.8
63.2
0.0853
81.7
70.4
<.0001***
Black
22.0
29.9
12.7
22.4
Other
5.3
6.9
5.6
7.2
Ethnicity (%)
Hispanic
7.3
14.6
0.0073**
10.4
15.2
0.0064**
Non-Hispanic
92.7
85.4
89.6
84.8
Gender (%)
Male
45.9
42.36
0.4484
41.5
45.3
0.1762
Female
54.1
57.6
58.5
54.7
Marital Status (%)
Married
70.7
60.8
0.1471
83.1
68.6
<.0001***
Divorced
23.6
30.4
13.1
25.8
Never married
5.8
8.8
3.9
5.7
Education (years completed)
12.0
11.2
0.0025**
13.0
11.6
<.0001***
Socioeconomic characteristics and employment
Respondent income ($)
17,712
14,396
0.7157
41,328
17,279
0.0033**
Household income ($)
36,829
30,062
0.119
79,372
33,277
<.0001***
Total household assets ($)
234,448
215,537
0.749
546,320
182,006
<.0001***
Working for pay (%)
5.1
9.0
0.0791
55.1
7.8
<.0001***
Total years worked (mean)
29.1
25.1
0.0018**
35.6
31.6
<.0001***
Health characteristics and health behaviors
Self-reported prob of a work-limiting health problem in next
decade (%)
73.3
57.5
0.5538
44.6
52.5
0.4232
Health problems limit work (%)
93.9
89.4
0.0883
19.0
80.0
<.0001***
Ever had (%)

55
High blood pressure
70.1
75.5
0.2044
50.9
63.7
<.0001***
Lung disease
22
23.6
0.6831
5.5
15.2
<.0001***
Psychological problem
42.1
38.9
0.4957
14.5
32.7
<.0001***
Number of health conditions ever reported
3.2
3.4
0.2904
1.7
2.8
<.0001***
Body mass index (above 30 indicates obesity)
31.2
31.5
0.71
28.5
31.1
<.0001***
CESD mental health score
2
2.6
3.2
0.0083**
1.1
2.6
<.0001***
Hospital stay in previous two years (%)
40
45.1
0.275
17.0
39.6
<.0001***
Any doctor visit in previous two years (%)
96.8
93.1
0.0492
92.0
93.5
0.335
Out-of-pocket medical expenditures ($)
5,233
4,498
0.5759
2,865
3,913
0.0034**
Number of days/week of drinks with alcohol
0.6
0.6
0.9522
1.2
62.9
<.0001***
Number of drinks of alcohol per day
0.5
0.6
0.5099
0.8
0.5
0.0043**
1
We used a t-test to compare the difference in means and a chi-square test to assess the difference in distributions. When we test the difference in distribution,
the test statistic is shown in the category heading rather than for a particular variable.
2
Center for Epidemiological Studies Depression (CESD) is an 8-point battery.
Notes: ***p<0.001; **p<0.01; *p<0.05. All values are taken at the ages 55 or 63, respectively, and all dollar values are inflated-adjusted to 2020 dollars.
Results for all other age groups available upon request.
Source: Authors’ calculations using the RAND-HRS and SSA data linkage.

56
Appendix Table B.4. Comparison of Characteristics of Respondents Who Correctly Report and Misreport Receipt of SSDI Benefits at
Age 63-64 (Linked Respondents, Unweighted)
Correct
Positive
False
Positive
p-value
1
Correct
Negative
False
Negative
p-value
1
Demographic characteristics
Race (%)
White
45.3
51.7
0.6005
81.3
53.4
<.0001***
Black
43.2
3500.0
13.3
38.6
Other
11.6
13.3
5.5
8.0
Ethnicity (%)
0.0
0.0
Hispanic
22.1
21.7
0.9488
10.0
28.4
<.0001***
Non-Hispanic
77.9
78.3
90.0
71.6
Gender (%)
0.0
0.0
Male
24.2
33.3
0.2166
42.6
30.7
0.0251
Female
75.8
66.7
57.4
69.3
Marital Status (%)
0.0
0.0
Married
30.8
61.7
0.0041*
82.3
38.7
<.0001***
Divorced
46.2
31.9
13.9
46.8
Never married
23.1
6.4
3.8
14.5
Education (years completed)
10.1
11.3
0.0238*
13.0
9.1
<.0001***
Socioeconomic characteristics and employment
Respondent income ($)
0
18,167
N/A
40,731
9,125
0.2118
Household Income ($)
11,486
28,336
<.0001***
75,058
12,775
<.0001***
Total Household assets ($)
39,800
256,063
0.1072
512,484
52,141
0.0025**
Working for pay (%)
0
5
0.0278**
49.8
3.4
<.0001***
Total years worked (mean)
15.5
21.9
0.009**
35.4
14.7
<.0001***
Health characteristics and behaviors
Health problems limit work
84.0
98.2
0.0065**
26.4
74.7
<.0001***
Self-reported probability (%):
Living to age 75
47.4
55.3
0.1948
65.7
44.6
<.0001***
Working full-time after age 65
3.0
0.4
0.1732
29.6
4.9
<.0001***

57
Ever had (%)
High Blood Pressure
77.9
68.3
0.1875
52.7
69.3
0.0019**
Diabetes
39.0
38.3
0.9396
19.3
37.5
<.0001***
Lung disease
28.4
16.7
0.0957
7.1
13.6
0.0179*
Heart disease
39.4
38.3
0.8993
16.7
38.6
<.0001***
Stroke
22.1
15.0
0.2784
4.8
14.8
<.0001***
Number of health conditions ever reported
3.6
3.2
0.1722
1.8
3.2
<.0001***
Body mass index (above 30 indicates obesity)
32.0
29.4
0.0524
28.8
32.0
<.0001***
CESD mental health score
2
3.5
3.4
0.8099
1.3
3.5
<.0001***
Number of ADL difficulties
3
1.2
1.3
0.705
0.2
1.1
<.0001***
Hospital stay in previous two years (%)
44.2
36.7
0.3561
19.7
36.4
<.0001***
Any doctor visit in previous two years (%)
92.6
93.3
0.8694
92.4
92.1
0.8989
Number of doctor visits in previous two years (%)
17.3
18.9
0.7617
9.1
18.4
<.0001***
Out-of-pocket medical expenditures ($)
1,201
4,130
0.0034**
3,185
375
0.0004***
Ever drank alcohol (%)
23.2
50.0
0.0005***
55.3
25.0
<.0001***
Number of drinks of alcohol per day
0.4
1.0
0.0096**
0.8
0.5
0.0358
1
We used a t-test to compare the difference in means and a chi-square test to assess the difference in distributions. When we test the difference in distribution,
the test statistic is shown in the category heading rather than for a particular variable.
2
Center for Epidemiological Studies Depression (CESD) is an 8-point battery.
3
Activities of Daily Living (ADLs) marked 0-5 to represent the number of ADLs in which the respondent reports at least some difficulty.
Notes: ***p<0.001; **p<0.01; *p<0.05. All values are taken at the ages 55 or 63, respectively, and all dollar values are inflated-adjusted to 2020 dollars.
Results for all other age groups available upon request.
Source: Authors’ calculations using the RAND-HRS and SSA data linkage.

58
RECENT WORKING PAPERS FROM THE
CENTER FOR RETIREMENT RESEARCH AT BOSTON COLLEGE
Changes in New Disability Awards: Understanding Trends and Looking Ahead
Lindsay Jacobs, December 2021
The Influence of Early-Life Economic Shocks on Aging Outcomes: Evidence from the U.S.
Great Depression
Valentina Duque and Lauren L. Schmitz, December 2021
Are There “Hot Spots” of Primary Impairments among New SSDI Awardees – and Do We
Know Why?
Jody Schimmel Hyde, Anna Hill, Jonathan Schwabish, and Aaron R. Williams, December 2021
Understanding the Local-Level Predictors of Disability Program Flows: New Adult Awards
and Beneficiary Work Activity
Jody Schimmel Hyde, Jonathan Schwabish, Paul O’Leary, and Dara Lee Luca, December 2021
Do Retirees Want Constant, Increasing, or Decreasing Consumption?
Anqi Chen and Alicia H. Munnell, December 2021
How Do Households Adjust Their Earnings, Saving, and Consumption After Children
Leave?
Andrew G. Biggs, Anqi Chen, and Alicia H. Munnell, November 2021
How Will COVID-19 Affect Pensions for Noncovered Workers?
Jean-Pierre Aubry, Kevin Wandrei, and Laura D. Quinby, November 2021
Is Demand for Older Workers Adjusting to an Aging Labor Force?
Damir Cosic and C. Eugene Steuerle, November 2021
How Does Debt Shape Health Outcomes for Older Americans?
Stipica Mudrazija and Barbara A. Butrica, November 2021
The Relationship Between Disability Insurance Receipt and Food Insecurity
Barbara A. Butrica, Stipica Mudrazija, and Jonathan Schwabish, November 2021
How to Increase Usage of SSA’s Online Tools
Jean-Pierre Aubry and Kevin Wandrei, November 2021
Work-Related Overpayment and Benefit Suspension Experiences of Federal Disability
Beneficiaries
Marisa Shenk and Gina Livermore, November 2021
All working papers are available on the Center for Retirement Research website
(https://crr.bc.edu) and can be requested by e-mail (crr@bc.edu) or phone (617-552-1762).
