
SCIENTIFIC ADVICE
Public health guidance on
screening and vaccination for
infectious diseases in newly
arrived migrants within the EU/EEA
www.ecdc.europa.eu

ECDC SCIENTIFIC ADVICE
Public health guidance on screening and
vaccination for infectious diseases in
newly arrived migrants within the EU/EEA
ii
This report from the European Centre for Disease Prevention and Control (ECDC) was coordinated by Teymur Noori, with the support
of Marieke J. van der Werf, Tarik Derrough, Erika Duffell, Anastasia Pharris, Jonathan Suk, Helena de Carvalho Gomes, Otilia Mårdh,
César Velasco Muñoz, Sara Causevic, Rikke Thoft Nielsen, Takis Panagiotopoulos, Agoritsa Baka, Andrew Amato, Johanna Takkinen,
Jan Semenza, Maarit Kokki, Josep Jansa, Piotr Kramarz, Denis Coulombier and Vicky Lefevre.
Acknowledgements
The first draft of this guidance was produced under Framework Service Contract Number ECDC/2015/016 with Euro Health Group A/S by
a team of independent consultants including Kevin Pottie, Rachael Morton, David Ingleby, Chris Greenaway, Charles Hui, Ana Requena-
Méndez, Eric Agbata, Tamara Lofti, Daniel Myran, Matthew Driedger, Alain Mayhew, Prinon Rahman, Peter Tugwell, Vivian Welch, Jessica
Dunn, Tatum McLeod, Harneel Kaur, Christine Mathew, Olivia Magwood and William Stauffer. In addition, ECDC would like to
acknowledge the following guideline GRADE methodologists for supporting the development of this guidance: Holger Schunemann, Elie
Akl, Pablo Alonso-Coello, Peter Tugwell, Robin Christensen, Vivian Welch and Joerg Meerpohl.
ECDC would like to acknowledge the support and guidance provided by members of the ECDC ad hoc scientific panel established to
support the development of this guidance: Angel Kunchev (Bulgaria), Gabrielle Jones (France), Anna Kuehne (Germany), Andreas
Gilsdorf (Germany), Agoritsa Baka (Greece), Lelia Thornton (Ireland), Francesco Castelli (Italy), Silvia Declich (Italy), Pierluigi Lopalco
(Italy), Maria van den Muijsenbergh (Netherlands), Machiel Vonk (Netherlands), Henrique Barros (Portugal), Sonia Dias (Portugal), Maria
Axelsson (Sweden), Rebecca Hall (United Kingdom), Manish Pareek (United Kingdom), Katherine Russell (United Kingdom), Ines
Campos-Matos (United Kingdom), Dominik Zenner (United Kingdom), Manuel Carballo (Switzerland) and Apostolos Veizis (Greece).
ECDC would also like to acknowledge the support and guidance provided by the ECDC advisory group that was established to support
the development of this guidance. The advisory group included the ad hoc scientific panel as well as experts and observers as follows:
Karin Taus (Austria) Cliona M Cheallaigh (Ireland), Núria Serre Delcor (Spain), Sally Hargreaves (United Kingdom), Hilary Kirkbride
(United Kingdom), Alison Crawshaw (United Kingdom), Isabel De La Mata (European Commission), Ludovica Banfi (European Union
Agency for Fundamental Rights), Olga Gorbacheva and Jenna Iodice (International Organisation for Migration), Denis Onyango (Africa
Advocacy Foundation), Kathy Attawell and Andreas Sandgren (independent consultants), Alexandra Ortega (International Panel
Physicians Association), and Joao Pires and Santino Severoni (World Health Organization, Regional Office for Europe).
ECDC would also like to acknowledge the Cochrane and Campbell Equity Methods Group and the following researchers for supporting
the systematic evidence reviews, GRADE evidence profiles and GRADE evidence to decision tables: Npur Abou-Chakra, Eric Agbata,
Nora Ahmad, Elie A Akl, Balqis Alabdulkarim, Pablo Alonso-Coello, Julia Del Amo, Henrique Barros, Beverley-Ann Biggs, Zeno Bisoffi,
Emmanuel Bottieau, Alison Brown, Manuel Carballo, Francesco Castelli, Robin Christensen, Sarah Crispo, Tarik Derrough, Sonia Dias,
Matthew Driedger, Erika Duffell, Jessica Dunn, Jui-Hsia Ray Hung, Gillian Gibson, Olga Gorbacheva, Christina Greenaway, Doug
Gruner, Rebecca Hall, Pamela Howeiss, Charles Hui, Harneel Kaur, Lama Kilzar, Tamara Lotfi, Olivia Magwood, Christine Mathew,
Alberto Matteelli, Alain Mayhew, Ted McConnell, Tatum McLeod, Rachael L Morton, Manish Pareek, Kevin Pottie, Teymur Noori, Iuliia
Makarenko, Joerg Meerpohl, Luisa Menjivar Ponce, Daniel Myran, Anastasia Pharris, Prinon Rahman, Ana Requena-Méndez, Nesrine
Rizk, Nick Rowbotham, Monica Sandu, Thierry Sangou, Lukas P Straub, Lelia Thornton, Anh Tran, Peter Tugwell, Andreas Sandgren,
Brittany Scarfo, Irene Veldhuijzen, Moneeza Walji, Vivian Welch, Marieke J. van der Werf, Dominik Zenner. Chris Greenaway led the
systematic reviews related to active TB, LTBI and hepatitis C and drafted those chapters in this guidance. Kevin Pottie led the
systematic review and provided an initial draft of the chapter on HIV. Daniel Myran led the systematic review and provided an initial
draft of the chapter on hepatitis B. Ana Requena and Eric N. Agbata led the systematic review and provided an initial draft of the
chapter on schistosomiasis and strongyloidiasis. Charles Hui and Jessica Dunn led the systematic review and provided an initial draft
of the chapter on vaccine-preventable diseases. Eric N. Agbata is a doctoral candidate for PhD in Methodology of Biomedical
Research and Public Health (Department of Paediatrics, Obstetrics, Gynaecology and Preventive Medicine), Universidad Autònoma de
Barcelona, Barcelona, Spain. His contributions to the section on schistosomiasis and strongyloidiasis guidance will form part of his
thesis.
ECDC would especially like to acknowledge David Ingleby for supporting ECDC in drafting Sections 2.1 (Recent trends of migration to
the EU/EEA) and 2.2 (Origin of migrants to the EU/EEA), Ludovica Banfi and Adriano Silvestri (European Union Agency for
Fundamental Rights) for drafting Section 2.3 (migrants’ access to health services), and Manish Pareek, Maria van den Muijsenbergh,
Sally Hargreaves and Teymur Noori for drafting Section 5.2 (linkage to care); Laura Nellums provided additional input.
ECDC would like to acknowledge the following migrant health experts for taking time to review the draft guidance: Denis Onyango
(Africa Advocacy Foundation) and Stephan Dressler (European AIDS Treatment Group), Alyna Smith (PICUM), István Szilárd
(University of Pecs), Irene Veldhuijzen (RVIM), Ines Campos-Matos (Public Health England), William Stauffer (University of
Minnesota), Benjamin Cowie (University of Melbourne) and Laura Nellums (Imperial College London).
ECDC would like to acknowledge Sally Hargreaves (St George’s, University of London) for her significant contribution in supporting
the generation of this guidance.
This guidance document was drafted by ECDC in accordance with Article 6(1) of Regulation (EC) No 851/2004 of the European
Parliament and of the Council of 21 April 2014, establishing a European Centre for Disease Prevention and Control.
ECDC issued this guidance document on its own initiative in accordance with Article 7(1) of Regulation (EC) No 851/2004. In the
framework of ECDC’s mandate, the specific purpose of ECDC guidance documents is to present different evidence-based statements
on a certain matter with their respective advantages and disadvantages. The responsibility for the choice of which option to pursue
and which actions to take, including the adoption of mandatory rules or guidelines, lies exclusively with the Member States. In its
activities, ECDC strives to ensure its independence, high scientific quality, transparency and efficiency.
Suggested citation: European Centre for Disease Prevention and Control. Public health guidance on screening and vaccination for
infectious diseases in newly arrived migrants within the EU/EEA. Stockholm: ECDC; 2018.
Stockholm, November 2018
ISBN 978-92-9498-280-3
doi: 10.2900/154411
Catalogue number TQ-04-18-919-EN-N
© European Centre for Disease Prevention and Control, 2018
Reproduction is authorised, provided the source is acknowledged.

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
iii
Contents
Abbreviations ...................................................................................................................................................... v
Glossary .............................................................................................................................................................. vi
Executive summary.............................................................................................................................................. 1
1. Introduction .................................................................................................................................................... 4
1.1 Target populations and definitions ............................................................................................................ 4
1.2 Rationale and objective of the guidance .................................................................................................... 4
1.3 Scope of the guidance .............................................................................................................................. 4
1.4 Target audience for the guidance.............................................................................................................. 5
2. Background ..................................................................................................................................................... 6
2.1 Migrants and infectious diseases in the EU/EEA ......................................................................................... 6
2.2 Recent trends in migration to the EU/EEA ................................................................................................. 6
2.3 Origins of migrants ................................................................................................................................... 7
2.4 Migrants’ access to health services ............................................................................................................ 7
3. Guidance development .................................................................................................................................... 9
3.1 Background .............................................................................................................................................. 9
3.2 Establishment of an ad hoc scientific panel ................................................................................................ 9
3.3 Selection of key infectious diseases and key questions .............................................................................. 9
3.4 Development of evidence reviews ........................................................................................................... 10
3.5 GRADE approach to develop evidence statements ................................................................................... 11
3.6 FACE survey ........................................................................................................................................... 12
3.7 Evidence review process and guideline development ............................................................................... 12
4. Conclusions ................................................................................................................................................... 13
4.1 Active tuberculosis .................................................................................................................................. 14
4.2 Latent tuberculosis infection ................................................................................................................... 19
4.3 HIV ........................................................................................................................................................ 23
4.4 Hepatitis B ............................................................................................................................................. 28
4.5 Hepatitis C ............................................................................................................................................. 33
4.6 Strongyloidiasis and schistosomiasis ........................................................................................................ 38
4.7 Vaccine-preventable diseases.................................................................................................................. 46
5. Implications for public health practice and research ........................................................................................ 52
5.1 Public health practice .............................................................................................................................. 52
5.2 Linkage to care....................................................................................................................................... 52
5.3 Research gaps ........................................................................................................................................ 53
6. Next steps ..................................................................................................................................................... 54
References ........................................................................................................................................................ 55
Annex 1. Top ten countries of birth of immigrants to the EU/EEA (average of 2014, 2015 and 2016) ................... 69
Annex 2. Top ten origins (nationalities) of asylum seekers in the EU/EEA (average of applications in 2015, 2016 and 2017) ... 72
Annex 3. Terms of reference of the ad hoc scientific panel.................................................................................. 76

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
iv
Figures
Figure 1. Annual immigration to the EU/EEA, 2008–2017 ...................................................................................... 6
Figure 2. WHO global map of TB incidence ......................................................................................................... 14
Figure 3. UNAIDS global map of HIV prevalence ................................................................................................. 23
Figure 3. Estimations of worldwide prevalence of chronic hepatitis B virus infection ............................................. 28
Figure 4. Prevalence of anti-HCV globally in 2015 ............................................................................................... 33
Figure 5. Distribution of schistosomiasis, worldwide (2012) ................................................................................. 39
Figure 6. Countries where schistosomiasis is endemic ......................................................................................... 42
Figure 7. Countries where strongyloidiasis is endemic ......................................................................................... 43
Figure 8. Distribution of measles cases by country, EU/EEA, 1 January–31 December 2017 ................................. 46
Figure 9. Measles vaccination coverage by country, EU/EEA countries, 2017 ....................................................... 47
Tables
Table 1. Eligibility criteria used for all diseases ................................................................................................... 10
Table 2. Interpretation of GRADE certainty of evidence....................................................................................... 11
Table 3. Interpretation of GRADE strength of recommendation ........................................................................... 12
Table 4. Constructs of the FACE survey .............................................................................................................. 12
Table 5. Evidence synthesis and guidance for active TB screening in migrants ..................................................... 17
Table 6. Active TB screening recommendations for migrants in selected low-TB-incidence countries .................... 18
Table 7. Evidence synthesis and guidance for LTBI screening in migrants ........................................................... 21
Table 8. LTBI screening recommendations for migrants in selected low-TB-incidence countries ........................... 22
Table 9. Evidence synthesis and guidance for HIV testing in migrants ................................................................. 26
Table 10. HIV screening recommendations for migrants in selected low-HIV-prevalence countries ....................... 26
Table 11. Evidence synthesis and guidance for hepatitis B vaccination and screening in migrants ........................ 31
Table 12. HBV screening recommendations for migrants in selected counties ...................................................... 32
Table 13. Evidence synthesis and guidance for hepatitis C screening in migrants ................................................. 36
Table 14. Hepatitis C screening recommendations for migrants in selected low-HCV-prevalence countries ............ 37
Table 14. Evidence synthesis and guidance for strongyloidiasis and schistosomiasis screening in migrants ........... 44
Table 15. Other international guideline recommendations for parasites for refugee and/or other migrant
populations ....................................................................................................................................................... 45
Table 16. Evidence synthesis and guidance for VPDs in migrant populations ....................................................... 50
Table 17. International guideline VPD recommendations for refugees and/or other migrant populations .............. 51
Table A-1. Composition of the ad hoc scientific panel ......................................................................................... 76

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
v
Abbreviations
AIDS Acquired immunodeficiency syndrome
ART Antiretroviral therapy
BCG Bacillus Calmette–Guerin vaccine
CDC US Centers for Disease Control and Prevention
CHB Chronic hepatitis B
CXR Chest X-ray
DALY Disability-adjusted life year
DTaP-IPV-Hib Diphtheria, tetanus, pertussis, polio, and Haemophilus influenzae type b
EACS European AIDS Clinical Society
EASL European Association for the Study of the Liver
EU/EEA European Union/European Economic Area
ELISA Enzyme-linked immunosorbent assay
GRADE Grading of recommendations assessment, development and evaluation
HBcAb Hepatitis B core antibody
HBsAg Hepatitis B surface antigen
HBV Hepatitis B virus
HCC Hepatocellular carcinoma
HCV Hepatitis C virus
HIC High-income country
HIV Human immunodeficiency virus
ICER Incremental cost–effectiveness ratio
INH Izoniazid
LMIC Low- and middle-income countries
LTBI Latent tuberculosis infection
MMR Measles, mumps, rubella vaccination
MSM Men who have sex with men
MTCT Mother-to-child transmission
NAT Nucleic acid test
NGO Non-governmental organization
PCR Polymerase chain reaction
PEG-IFN Pegylated interferon
PICO Population, intervention, comparison, outcome
PMTCT Prevention of mother-to-child transmission
PWID People who inject drugs
QALY Quality-adjusted life year
RBV Ribavirin
RIF Rifampicin
RCT Randomised controlled trial
RDT Rapid diagnostic test
TB Tuberculosis
TST Tuberculin skin test
UN United Nations
UNAIDS Joint United Nations Programme on HIV/AIDS
VCT Voluntary counselling and testing
VPD Vaccine-preventable diseases
WHO World Health Organization

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
vi
Glossary
Acceptability How acceptable the intervention is to the target population in relation to the effect.
Asylum seeker A person who awaits a decision on the application for refugee status under
relevant international and national instruments.
Cost-effectiveness The extent to which an intervention or prevention programme is effective in
relation to its costs, e.g. euro cost per life-years gained.
Feasibility Ability to implement an intervention in terms of time, money, or other
circumstances.
GRADE working group The GRADE Working Group has developed a common, sensible and transparent
approach to grading quality (or certainty) of evidence and strength of
recommendations. The GRADE approach is now considered the standard in
guideline development.
Health Health is a state of complete physical, mental and social well-being and not merely
the absence of disease or infirmity (1).
Health equity Health equity is the absence of avoidable or remediable health differences among
groups of people, whether those groups are defined socially, economically,
demographically, or geographically.
Irregular migrant Is a person who, owing to unauthorised entry, breach of a condition of entry, or
the expiry of his or her visa, lacks regular status in a transit or host country. The
definition also covers those persons who have entered a transit or host country
lawfully but have stayed for a longer period than authorised or subsequently taken
up unauthorised employment.
Migrant A migrant, as defined by the United Nations, is any individual who lives in a
country temporarily or permanently apart from his or her usual place of residence
for at least a year (2). In the EU/EEA context, migrants include both internal
European migrants living outside of their European country of birth, and external
migrants originating from outside of the EU/EEA.
Newly arrived migrants Newly arrived migrants are defined in this guidance as individuals who have
migrated to a host country within the EU/EEA in the past five years.
Pre-entry screening Pre-entry migrant screening refers to migrant screening programmes operating in
migrant departure countries, for example for migrants applying for work visas.
Refugee A person who, owing to a well-founded fear of persecution for reasons of race,
religion, nationality, membership of a particular social group or political opinions, is
outside the country of his or her nationality and is unable or, owing to such fear, is
unwilling to avail himself of the protection of that country (3).

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
1
Executive summary
Increased rates of migration to and within the European Union and European Economic Area (EU/EEA) in recent years
has made the development of migration policy, including health policy, a priority for the region. A migrant is defined as
any individual who lives in a country temporarily or permanently away from his or her usual place of residence for at
least a year. Migrants do not generally pose a health threat to the host population. However, some subgroups of
migrants, including refugees, asylum seekers, and irregular migrants are particularly vulnerable to infectious diseases
and may have worse health outcomes than the host population. In a number of EU/EEA Member States, subgroups of
migrant populations are disproportionately affected by infectious diseases such as tuberculosis, HIV, and hepatitis B
and C. Consequently, screening and vaccination programmes may be of benefit for newly arrived migrants, i.e. those
who have arrived in the EU/EEA within the past five years
1
.
The European health policy framework ‘Health 2020’ aims to ‘significantly improve the health and well-being of
populations, reduce health inequalities, strengthen public health and ensure people-centred health systems that are
universal, equitable, sustainable and of high quality’. ECDC has sought to support this aim in migrant health by developing
evidence-based guidance on the prevention of infectious diseases among newly arrived migrants in the EU/EEA.
Objective, method and approach
The main objective of this guidance is to provide scientific advice, based on an evidence-based assessment of
targeted public health interventions, to facilitate effective screening and vaccination for priority infectious diseases
among newly arrived migrant populations to the EU/EEA. It is intended to support EU/EEA Member States to develop
national strategies to strengthen infectious disease prevention and control among migrants and meet the health
needs of these populations.
The guidance has been developed using a series of systematic evidence reviews and the grading of recommendations
assessment, development and evaluation (GRADE) evidence-to-decision framework, as well as drawing on the
opinions of an ad hoc scientific panel through a consultation and assessment process. ECDC appointed a scientific
panel consisting of 21 experts from EU/EEA Member States to review the evidence and express opinions on the
evidence-based statements that relate to vulnerable migrant groups. None of the members of the panel declared any
conflicts of interest with regard to the topic and their participation in the panel. In addition to the scientific panel,
ECDC established an advisory group of experts in infectious disease, public health and migration to participate in
meetings in order to select the key infectious diseases for which guidance is needed and to support the review
process.
The advisory group and ad hoc scientific panel selected the following key infectious diseases for consideration: active
tuberculosis (TB) and latent TB infection (LTBI), HIV, hepatitis B (HBV), hepatitis C (HCV), vaccine-preventable
diseases (measles, mumps, rubella, diphtheria, tetanus, pertussis, polio, Haemophilus influenzae type B,
strongyloidiasis, and schistosomiasis.
Key overarching questions were:
• Should newly arrived migrants be offered screening for active TB, LTBI, HIV, hepatitis B, hepatitis C,
strongyloidiasis, and schistosomiasis? Who should be targeted and how?
• Should newly arrived migrants be offered vaccination for measles, mumps, rubella, diphtheria, tetanus,
pertussis, polio, Haemophilus influenzae type B (HiB) and hepatitis B?
• What are the implementation considerations in EU/EEA countries?
The approach involved developing key research questions (PICO: population, intervention, comparison, outcome) and
an analytic framework to identify key steps and questions related to evidence of effectiveness along the screening–
intervention pathway, in order to formulate search strategies and identify relevant literature.
Search terms and strategies appropriate for each infectious disease were used to search for published literature in
PubMed, the Cochrane Database of Systematic Reviews, and Embase from January 2005 to May 2016; grey literature
and existing guidelines were also identified. In developing the guidance, ECDC sought to build on existing systematic
reviews and randomised controlled trials; in addition, newly developed additional evidence reviews were used to
address gaps in the evidence base. The systematic reviews that underpin this guidance were conducted in line with
PRISMA
2
reporting guidelines.
1
Screening in this document implies a voluntary action that should be linked to an appropriate intervention; for example,
treatment, vaccination, health education.
2
PRISMA is an evidence-based minimum set of items for reporting in systematic reviews and meta-analyses. PRISMA focuses on
the reporting of reviews evaluating randomized trials, but can also be used as a basis for reporting systematic reviews of other
types of research, particularly evaluations of interventions. http://www.prisma-statement.org/

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
2
The GRADE evidence-to-decision approach was used to frame evidence and develop statements, and to rate the
strength of the evidence-based statements. Evidence-based statements were developed and graded through an
iterative consensus process with the advisory group and ad hoc scientific panel. The ad hoc scientific panel members
completed a FACE survey (feasibility, acceptability, cost and equity), which was used to inform the guidance. GRADE
Pro Panel Voice Software
3
was used to review statements and vote on all evidence-to-decision criteria. The evidence
review and guideline development process consisted of three rounds of review: of the evidence review findings, the
draft evidence-based statements, and the draft guidance.
Results
This guidance focuses on newly arrived migrants within the EU/EEA, taking into consideration country of origin,
circumstances of migration, and age and gender, where relevant.
Available evidence suggests that it likely to be effective and cost-effective to screen child, adolescent and adult migrants for
active TB and LTBI, HIV, HCV, HBV, strongyloidiasis and schistosomiasis, and that there is a clear benefit to enrolling
migrants in vaccination programmes and ensuring catch-up vaccination where needed. This is, however, often conditional
on the burden of disease in migrants' countries of origin. Box 1 summarises the key evidence-based statements.
Box 1. Summary of evidence-based statements for screening and
vaccination for infectious diseases among newly arrived migrants
Active TB
Offer active TB screening using chest X-ray (CXR) soon
after arrival for migrant populations from high-TB-
incidence countries. Those with an abnormal CXR should
be referred for assessment of active TB and have a
sputum culture for Mycobacterium tuberculosis.
Latent TB infection
4
Offer LTBI screening using a tuberculin skin test (TST) or
an interferon-gamma release assay (IGRA) soon after
arrival for all migrant populations from high-TB-incidence
countries and link to care and treatment where indicated.
HIV
Offer HIV screening to migrants who have lived in
communities with high HIV prevalence (≥1%). If HIV
positive, link to care and treatment as per clinical guidelines.
Offer testing for HIV to all adolescents and adult
migrants at high risk for exposure to HIV. If HIV positive,
link to care and treatment as per clinical guidelines.
Hepatitis B
Offer screening and treatment for hepatitis B (HBsAg and
anti-HBc, anti-HBs) to migrants from intermediate/high
prevalence countries (≥2% to ≥5% HBsAg.)
Offer hepatitis B vaccination series to all migrant children
and adolescents from intermediate/high prevalence
countries (≥2% to ≥5% HBsAg) who do not have
evidence of vaccination or immunity.
Hepatitis C
Offer hepatitis C screening to detect HCV antibodies to
migrant populations from HCV-endemic countries (≥2%)
and subsequent RNA testing to those found to have
antibodies. Those found to be HCV RNA positive should
be linked to care and treatment.
Schistosomiasis
Offer serological screening and treatment (for those
found to be positive) to all migrants from countries of
high endemicity in sub-Saharan Africa, and focal areas of
transmission in Asia, South America and North Africa
(see Figure 14).
Strongyloidiasis
Offer serological screening and treatment (for those
found to be positive) for strongyloidiasis to all migrants
from countries of high endemicity in Asia, Africa, the
Middle East, Oceania and Latin America (see Figure 15).
Vaccine-preventable diseases
Offer vaccination against measles/mumps/rubella (MMR)
to all migrant children and adolescents without
immunisation records as a priority.
Offer vaccination to all migrant adults without
immunisation records with either one dose of MMR or in
accordance with the MMR immunisation schedule of the
host country.
Offer vaccination against diphtheria, tetanus, pertussis,
polio and HiB (DTaP-IPV-Hib)
56
to all migrant children and
adolescents without immunisation records as a priority.
Offer vaccination to all adult migrants without
immunisation records in accordance with the
immunisation schedule of the host country. If this is not
possible, adult migrants should be given a primary series
of diphtheria, tetanus, and polio vaccines.
For the evidence-based statement on hepatitis B
vaccination, please see Section 4.4.
3
Panel Voice is an add-on to the GRADEpro software that supports panel groups during the guideline development process and
facilitates online and asynchronous decision making. Available from: https://gradepro.org
4
See recent ECDC guidance on programmatic management of LTBI in the European Union for further guidance on management.
Available from: https://ecdc.europa.eu/sites/portal/files/documents/LTBI%20cost-effectiveness%20report.pdf
5
Diphtheria, tetanus, pertussis, polio, and Haemophilus influenzae type b
6
Vaccination against Hib is only recommended to children up to five years of age.

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
3
Implementation considerations
Infectious diseases screening and vaccination programmes for migrants to the EU/EEA should be consistent with
public health principles. The success of these interventions depends on both the provision of healthcare services
that are responsive to the needs of migrants and the ability of migrant populations to access key services. Key
implementation considerations for infectious disease screening and vaccination programmes targeting newly
arrived migrants include:
• Ensure all screening and vaccination is voluntary, confidential, non-stigmatising and carried out for the
benefit of the individual.
• Provide screening, referral, and linkage to care and treatment for all individuals who require it.
• Address the individual, community and health system barriers (for example, low risk perception; disease-
related stigma; socio-economic, cultural and linguistic barriers; lack of entitlement to healthcare or to free
healthcare) that limit migrants’ uptake of screening and vaccination, and subsequent uptake and completion
of treatment.
• Consider the unique needs of newly arrived migrants when offering screening and vaccination, in terms of
delays to presentation, follow-up appointments, and uptake and completion of treatment, and take steps to
reduce post-screening/testing drop-out from care.
• Recognise that newly arrived migrants face a range of issues (for example, housing, employment, mental
health problems) that may take precedence over seeking preventative healthcare and that may increase the
risks or consequences of infectious diseases.
The ad hoc scientific panel members strongly supported free screening, vaccination and care for key infectious
disease for all migrants in the EU/EEA, including irregular migrants.
Next steps
Public health programmes have an important role in improving the health and social determinants of health for
newly arrived migrants to the EU/EEA. Priority needs to be given to promoting uptake of screening and vaccination
and, in particular, to monitoring uptake of TB, HIV and hepatitis testing and linkage to care and treatment in high-
risk migrant populations.
Public health programmes may have to adapt their communication and approaches. Better understanding of
migrant perceptions about infectious diseases, screening, testing and vaccination, and the acceptability and
accessibility of healthcare services, is critical. Tailored approaches such as multiple testing, integrated care for
infectious diseases and other health needs, and migrant-friendly services, are also needed.
Since the vast majority of preventative and curative healthcare for migrant populations is provided by community-
based primary care services, there is a need to ensure that health professionals have sufficient knowledge of
migrant health needs and that they have skills in culturally sensitive health education, as well as access to
culturally and linguistically appropriate information materials and interpretation support services. Community
engagement, through culturally sensitive outreach programmes as well as community-based care, is also critical to
improving awareness and uptake of services among migrant populations. Community-based care can improve trust
and ease of access to screening and vaccination services. There is an opportunity to learn from the experience of
EU/EEA countries that are implementing effective programmes to reach newly arrived migrants through approaches
that include culturally competent health promotion and care and use of interpreters, training of community-based
primary care professionals, and collaboration with public health and migrant community coalitions.
The process of developing this guidance has highlighted gaps in evidence concerning infectious disease control and
vaccination in migrant populations. It has also detected limitations of the evidence on effective and cost-effective
delivery of prevention interventions targeting this population. Improvements in surveillance are required to increase
the completeness and quality of data and inform more accurate estimates of disease, morbidity and mortality
among migrant populations. Research is needed to provide strong evidence of the impact of interventions,
challenges around diagnosis and treatment, and more robust data on acceptability, effectiveness, and cost-
effectiveness of screening and vaccination programmes targeting migrants. More research, including community-
based participatory action research, is also needed on the determinants of health in migrant populations and
migrant community perspectives, as is research into multiple-disease screening and roles for screening in
community-based primary healthcare services.

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
4
1. Introduction
1.1 Target populations and definitions
An international migrant, as defined by the United Nations, is any individual who lives in a country temporarily or
permanently apart from his or her usual place of residence for at least a year (2). Migrant populations include
refugees, asylum seekers, and others who may have been forced to flee conflict, natural disasters, or economic
peril, irregular migrants who reside in the EU/EEA without regular status, and voluntary migrants who seek
economic opportunities (4). Some migrant populations may originate from countries where infectious diseases have
a high prevalence and/or may have experienced migration journeys that increase the risk of infection. The target
population for this guidance is newly arrived migrants, i.e. those who have migrated to the EU/EA within the past
five years, who may benefit from being offered screening and vaccination for infectious diseases. Targeting newly
arrived migrants also provides an important opportunity for public health and community interventions to prevent,
detect, and treat key infectious diseases (5 ).
1.2 Rationale and objective of the guidance
Public health programmes have played an important role in assessing migrants for infectious diseases. Historically,
port-of-entry authorities met ships on arrival and conducted screening and quarantine programmes (6). More
recently, the number of migrants and diverse modes of travel have reduced the effectiveness of this approach (7).
Consequently, evidence-based guidance focusing on migrant populations has been developed to guide and
influence public health policy and primary health assessments in countries including Australia, Canada, Ireland,
Italy, the United Kingdom (UK) and the United States (US) (5, 8-13). It is also clear that there is a need to improve
the delivery of health services and interventions to migrant populations (14). The failure to address migrant rights
to healthcare and access to health services, and to consider their unique needs, also risks undermining regional
and global efforts to combat the spread of communicable diseases (15, 16).
Many EU/EEA countries have had longstanding and stable migration patterns based on past relationships with
countries outside Europe. However, global migration patterns and flows are changing due to political, economic and
environmental instability. Migrants to the region are a diverse group, making it hard to generalise about their
health needs. However, some migrant populations are disproportionately affected by, or vulnerable to, certain
infectious diseases and have low levels of vaccination – reflecting the burden of disease and weak health systems
in countries of origin, exposure to infectious diseases while ‘en route’, and living conditions and barriers to
accessing health services after arrival to the EU/EEA (17).
This guidance aims to provide an evidence-based assessment of targeted public health interventions to facilitate
effective screening and vaccination for priority infectious diseases among newly arrived migrant populations to the
EU/EEA (6, 17). It is intended to support EU/EEA Member States to develop national strategies to strengthen
infectious disease prevention and control among migrants and to meet the health needs of this population. While
this guidance focuses on screening for infectious diseases and vaccination, it should be noted that certain migrant
populations also face an undue burden of non-communicable diseases, and health systems should take an
integrated approach to migrant health, ensuring it is non-stigmatising and carried out for the benefit of the
individual.
1.3 Scope of the guidance
This guidance document covers key infectious diseases selected by an ad hoc scientific panel: active tuberculosis
(TB) and latent TB infection (LTBI), HIV, hepatitis B, hepatitis C, vaccine-preventable diseases (measles, mumps,
rubella, diphtheria, tetanus, pertussis, polio, Haemophilus influenzae type B), strongyloidiasis, and schistosomiasis.
The scientific panel also took into consideration the following public health values and principles in the
development of the statements and guidance: relevance, effectiveness, cost-effectiveness, accessibility,
acceptability, feasibility, health equity and community participation.
The following published methods and evidence reviews, many of which focus on the effectiveness and cost-
effectiveness of vaccination or screening for these key infectious diseases, have provided the foundation for the
development of this guidance:
• Prevention and assessment of infectious diseases among children and adult migrants arriving to the
EU/EEA: a protocol for a suite of systematic reviews for public health and health systems (18).
• The effectiveness and cost-effectiveness of screening for active tuberculosis among migrants in the EU/EEA:
a systematic review (19).
• The effectiveness and cost-effectiveness of screening for latent tuberculosis among migrants in the EU/EEA:
a systematic review (20).

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
5
• The effectiveness and cost-effectiveness of screening for HIV in migrants in the EU/EEA: a systematic
review (21).
• Effectiveness and cost-effectiveness of screening for and vaccination against hepatitis B virus in migrants in
the EU/EEA: a systematic review (22).
• The effectiveness and cost-effectiveness of hepatitis C screening for migrants in the EU/EEA: a systematic
review (23).
• The effectiveness and cost-effectiveness of screening for schistosomiasis and strongyloidiasis in migrants in
the EU/EEA: a systematic review [in press].
• Intervention to improve vaccine uptake and cost-effectiveness of vaccination strategies in newly arrived
migrants in the EU/EEA: a systematic review (24).
• Evaluating the accessibility and acceptability of infectious disease interventions among migrants in the
EU/EEA: a systematic review (25).
• Linkage to care is important and necessary when identifying infections in migrants: journal article (26).
This guidance has been developed using the GRADE evidence-to-decision framework; it draws on the opinions of
an ad hoc scientific panel through a consultation and assessment process (18). Previous ECDC technical reports
related to migrant health have addressed prevalence and scientific advice on infectious diseases and vaccinations
(17, 27), but not in the form of a comprehensive evidence-based guidance document. This guidance does not
cover all interventions directly related to prevention, detection, and management of the key infectious diseases; we
suggest clinical guidance (i.e. WHO, EASL (European Association for the Study of the Liver), EACS (European AIDS
Clinical Society), etc.) be consulted for additional information.
1.4 Target audience for the guidance
The target audience for this guidance includes national, regional and international policymakers, public health and
healthcare planners, health researchers, health professionals, and civil society organisations working with migrant
populations. Any adaptation of this guidance should be based on a country-specific assessment that considers both
the numbers and types of arriving migrants, and the legal and organisational context in which national health
systems operate.

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
6
2. Background
2.1 Migrants and infectious diseases in the EU/EEA
Some migrant populations are at increased risk of specific infectious diseases, including active and latent TB, HIV,
hepatitis B and hepatitis C (17, 28). In addition, immunisation coverage is low in some migrant populations, making
them more susceptible to vaccine-preventable diseases (VPDs) (29-31). Factors that increase the vulnerability of
migrants to infectious diseases include: demographic profile, patterns of disease and weak health systems in
countries of origin, high-risk behaviour, exposure to perilous migration journeys that increase the risk of infectious
diseases, living conditions in host countries (such as reception centres, overcrowding or shared accommodation),
social, economic, cultural and legal barriers in host countries that limit or prevent access to and uptake of
healthcare services (28, 32 ). Social and economic barriers include stigma, discrimination and isolation, and
unemployment (4). Cultural and legal barriers include language, religion, health beliefs, and lack of entitlement to
healthcare or difficulties in accessing available entitlements (33). The vulnerability of migrant populations to
infectious diseases can also be exacerbated by poor living conditions and other determinants of health in the host
country (34-37).
2.2 Recent trends in migration to the EU/EEA
The EU/EEA comprises 31 Member States, with a total population of 517 million at the end of 2017. Migrants made
up 11% of this population in 2017, with 4% being born in another EU/EEA country and 7% originating from
outside the EU/EEA (38). ‘Short-term’ migrants (residing for between 3 and 12 months) are not included in
population statistics but, of all first residence permits issued in 2016, 39% were valid for less than a year (39). The
above figures are averaged over the EU/EEA, but it is important to note that there are considerable variations
between the Member States.
There are also fluctuations in the volume and type of migration to the EU/EEA from year to year. Figure 1 shows
annual totals of first residence permits issued, distinguishing between ‘routine’ reasons for migration (work, family,
education, ‘residence only’ and ‘other reasons not specified’) and international protection (refugee status,
subsidiary and humanitarian protection, unaccompanied minors and victims of trafficking) (40).
Figure 1. Annual immigration to the EU/EEA, 2008–2017
Source: Eurostat, Frontex and IOM (40).
Even during the large influx of unauthorised arrivals in 2015 and 2016, most migration to the EU/EEA was for
‘routine’ reasons. Following the financial crisis in 2007, routine immigration declined until 2012–2013, when it
started to rise again. Unauthorised landings (41) and asylum applicants (42) have increased steadily since 2012,
although they decreased as a result of the EU–Turkey deal in March 2016, when the main sea route shifted to
Italy (43).
As Figure 1 shows, many arrivals in 2015 did not lead to an asylum application until 2016; the backlog of
applications only started to decline in 2017. Totals for asylum applications in 2015 and 2016 have been adjusted to
0
500,000
1,000,000
1,500,000
2,000,000
2,500,000
3,000,000
2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
Routine permits (all)
Routine permits (≥ 12 months)
Asylum applications
Int. Protection (all)
Int. Protection (≥ 12 months)
Unauthorised landings

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
7
take account of repeat applications by the same person (estimated at 175 000 and 98 000, respectively) (44). In
the three years from 2015 to 2017, approximately 56% of the 2 672 000 asylum decisions were positive (45). Of
the asylum seekers whose applications were rejected, only about half can be expected to leave, adding
approximately 580 000 to the EU/EEA’s total number of irregular migrants (46)]. Between 2014 and 2017, 94% of
all migrants to the EU28 were hosted in the EU-15 countries (47); for those given international protection, the
proportion was 98% (45).
2.3 Origins of migrants
Patterns of recent migration to the EU/EEA reflect a range of geographical and historical factors, including
European colonialism, and conflicts, for example in Syria. In the 21st century, the number of countries from which
migrants to Europe originate has greatly increased. The available data (covering 56% of non-EU/EEA immigrants)
show that in 2014, 2015 and 2016, the largest numbers were from Syria (94 000), China (84 000), India (77 000),
Morocco (50 000) and the USA (43 000). Migrants originated from 190 different countries globally, 31 of which
were the source of more than 10 000 migrants a year. Data on the main countries of birth of immigrants (Annex 1)
and asylum seekers (Annex 2) arriving from outside of the EU/EEA is important to give primary healthcare workers
and policymakers an indication of which infectious diseases are prevalent in the countries of origin, which can
guide screening efforts at countries of destination.
As the prevalence of infectious diseases among newly arrived migrants tends to reflect the prevalence in countries
of origin, information about disease patterns in these countries can determine whether screening is justified. For
similar reasons, information about immunisation coverage in migrants’ countries of origin is also important.
2.4 Migrants’ access to health services
The right to health is a basic social right. Article 12 of the United Nations (UN) International Covenant on
Economic, Social and Cultural Rights, which has been ratified by all EU Member States, enshrines ‘the right of
everyone to the enjoyment of the highest attainable standard of physical and mental health’. According to the UN
Committee on Economic, Social and Cultural Rights – the body entrusted with supervising the application of the
Covenant – core obligations derived from this right apply to everyone and do not depend on the regular status of
the persons concerned (48). Therefore, they also apply to migrants, both regular and irregular. Target 3.8 of the
UN’s Sustainable Development Goal on health to provide ‘access to quality essential healthcare services, and access
to safe, effective, quality and affordable essential medicines and vaccines for all’, also applies to migrants.
Concerning the health of migrant children, both prenatal and postnatal, Article 24 of the UN Convention on the
Rights of the Child (CRC) provides specifically for children’s access to health services and obliges states to ‘ensure
appropriate prenatal and postnatal healthcare for mothers’ (49). The reference to adequate access to healthcare
for mothers is motivated by the strong impact that maternal morbidity and mortality may have on children’s health.
The CRC requires that Member States ensure the provision of necessary medical assistance and healthcare with an
emphasis on provision of primary healthcare (50). Article 12 [2] of the UN Convention on the Elimination of all
Forms of Discrimination against Women provides similar healthcare rights to pregnant women (51).
At the EU level, the Charter of Fundamental Rights of the European Union (the Charter) includes the right to
healthcare under Article 35, which states that ‘everyone has the right of access to preventive healthcare and the
right to benefit from medical treatment under the conditions established by national laws and practices’ (52). The
Charter’s application is limited to those matters that fall within the scope of EU law. In accordance with Article 168
of the Treaty on the Functioning of the European Union, the EU’s role in the field of health is limited to
complementing the national policies of the EU Member States, with a focus on improving public health and
increasing health security, including surveillance of communicable diseases.
EU secondary law regulates access to healthcare for a variety of categories of migrants:
• Applicants for international protection, commonly referred to as asylum applicants, are entitled to
necessary healthcare, which must include at least emergency care and essential treatment of illness, as well
as necessary medical or other assistance for those who have special needs.
• Persons granted international protection, namely refugees and subsidiary protection status holders,
have equal access to healthcare to that of a Member State national.
• Various EU law instruments contain a duty by Member States to address the urgent medical needs of
people intercepted or apprehended at the border, including those rescued at sea.
• Victims of trafficking in human beings are entitled to necessary medical treatment, including
psychological assistance, counselling and information.
• People in return procedures are entitled to the same level of healthcare granted to asylum applicants –
namely ‘emergency healthcare and essential treatment of illness’ – if they have been given a period for
voluntary departure or if their removal was formally postponed.

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
8
EU law does not regulate access to healthcare for migrants in an irregular situation if they do not fall under the
specific categories listed above. The level of access to healthcare provided to them differs significantly between EU
Member States. Evidence collected by the EU Agency for Fundamental Rights in 2010 showed that only four
Member States provided cost-free emergency, primary and secondary healthcare to this group (Belgium, France,
the Netherlands and Portugal). In two other countries, cost-free access was provided for emergency and primary
healthcare (the UK) or emergency and secondary healthcare (Italy). In the majority of EU Member States, access
to healthcare for migrants in an irregular situation is often conditional and restricted to a limited set of services
(‘emergency care’, ‘urgent medical aid’, ‘treatment that cannot be deferred’). Among the EU countries that provide
access only to emergency healthcare for migrants, nine require payment for the cost of the emergency healthcare
provided. Although in most cases emergency treatment would not be denied, the sums charged can be
considerable (53).
In the case of communicable diseases, almost all European countries provide migrants in an irregular situation with
access to screening services, but fewer countries provide access to state-funded treatment (54). For example, in
2017, laws and policies limited provision of HIV treatment for irregular migrants in more than half of EU/EEA
countries (55). Even when cost-free access to healthcare is provided, practical barriers may prevent migrants from
enjoying the right to healthcare. These include unawareness of entitlements, administrative requirements (e.g.
proof of lack of financial means; requirement to register with a general practitioner) and, for migrants in an
irregular situation, the fear that visits to healthcare services may be reported to immigration law enforcement
authorities. In some Member States, there are additional barriers such as the requirement to provide an identity
document or proof of residence in the host country or in a particular city (56).
Building on the international and European human rights law framework, the EU Agency for Fundamental Rights
has recommended that migrants in an irregular situation should, as a minimum, be entitled to necessary healthcare
services, which should include the option of seeing a general practitioner and receiving necessary medicines. There
have been calls for a more holistic and inclusive approach to migrant health to be adopted across the EU/EEA,
which recognises the health rights of migrants and works towards removing legal, social, and cultural barriers to
health services to improve the health of migrants (57).

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
9
3. Guidance development
3.1 Background
The European health policy framework 'Health 2020’ aims to ‘significantly improve the health and well-being of
populations, reduce health inequalities, strengthen public health and ensure people-centred health systems that
are universal, equitable, sustainable and of high quality’. In the area of migrant health, ECDC has sought to support
this through the development of evidence-based guidance for prevention of infectious diseases among newly
arrived migrants to the EU/EEA. The specific objective was to systematically review and synthesise the evidence on
infectious diseases screening and vaccination for newly arriving migrants. Using the newly developed GRADE
‘evidence-to-decision’ approach, ECDC reviewed evidence from high-quality systematic reviews on effectiveness,
acceptability, feasibility, equity, resource use and cost-effectiveness of migrant screening and vaccination (18).
3.2 Establishment of an ad hoc scientific panel
Setting priorities for public health interventions, particularly when dealing with diverse migrant populations and
limited health system resources, has been shown to improve health outcomes (58). There is no standard algorithm
to determine public health priorities, although burden of illness, feasibility and economic considerations are all
important factors (59, 60). At the outset, therefore, ECDC convened an advisory group consisting of EU/EEA clinical
and public health stakeholders in November 2015 to explore the scope, priorities and principles for developing this
guidance (61, 62).
Following this initial meeting, ECDC appointed an ad hoc scientific panel, including 21 experts from a range of
EU/EEA Member States (see panel members and terms of reference in Annex 3). The main purpose of the panel
was to review and assess the evidence base and provide consensus statements on good practices for interventions
and service models targeting vulnerable groups. ECDC’s process for setting up ad hoc scientific panels to provide
independent advice follows a strict methodology and includes the following steps: identification of experts;
collecting declarations of interest from experts; evaluating eligibility; and ruling out conflicts of interest of experts
through clearance by the ECDC compliance officer. At the end of this process, the ECDC Director formally appoints
the panel members.
The ad hoc scientific panel members for this guidance were identified through the ECDC Expert Directory,
suggestions from the ECDC Advisory Forum and ECDC experts, and a literature search for experts who have
published on this or related topics. Panel members were expected to have experience in critical appraisal of peer-
reviewed publications, familiarity with systematic review methods, the application of evidence to decision-making,
and expertise in disease prevention and health promotion. In deciding on the composition of the panel, ECDC also
took into account country representativeness and the specific expertise and experience of experts. All panel
members signed a declaration of interest, which was reviewed by the ECDC compliance officer. None of the
members of the panel declared any interests that were considered to be a conflict with regard to the topic and
their participation in the panel. Panel members were asked to provide opinions based on their professional and
scientific experience, and to do so on a personal basis as an independent expert, not representing the interests of
any commercial body, professional body or Member State. The ad hoc scientific panel was officially appointed by
the ECDC Acting Director in October 2016.
In addition to the ad hoc scientific panel, ECDC invited experts in infectious disease, public health, and migration to
participate in meetings to select the key infectious diseases and support the review process; these people, together
with the ad hoc scientific panel, formed the advisory group. The advisory group included representatives from the
European Commission, the WHO Regional Office for Europe, and the International Organisation for
Migration (IOM).
3.3 Selection of key infectious diseases and key questions
The following infectious diseases were prioritised for consideration: active TB, LTBI, HIV, hepatitis B, hepatitis C,
vaccine-preventable diseases (measles, mumps, rubella, diphtheria, tetanus, pertussis, polio, Haemophilus
influenzae type B), strongyloidiasis and schistosomiasis. Key overarching questions were:
• Should newly arrived migrants be offered screening for active TB, LTBI, HIV, hepatitis B, hepatitis C,
strongyloidiasis, and schistosomiasis? Who should be targeted and how?
• Should newly arrived migrants be offered vaccination for measles, mumps, rubella, diphtheria, tetanus,
pertussis, polio, Haemophilus influenzae type B (HiB)?
• What are the implementation considerations in EU/EEA countries?

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
10
Additional questions of relevance to each specific infectious disease are outlined in the registered systematic review
protocol (18).
3.4 Development of evidence reviews
With technical support from the Campbell and Cochrane Equity Methods Group
(http://methods.cochrane.org/equity/welcome) and members of the Grading of Recommendations Assessment,
Development and Evaluation (GRADE) Working Group, a series of systematic evidence reviews was undertaken for
each of the prioritised infectious disease areas (see Section 1.3). A detailed description of the methods for the
systematic reviews can be found in the registered systematic review protocol (18). In addition, four downloadable
supplements to this guidance are available on the ECDC website: the analytic framework, characteristics of
included studies for effectiveness and cost-effectiveness, PRISMA flow diagrams on (cost-)effectiveness, and the
GRADE profile tables specifying the certainty of evidence.
In summary, the approach involved developing key PICO (population, intervention, comparison, outcome)
questions (Table 1]. As anticipated (18) and based on previous work in developing guidance in the area of migrant
health (5), migrant populations are underrepresented in randomised controlled trials and other intervention
research. When available, studies on high-risk migrant groups were prioritised. However, when migrant-specific
studies were lacking, indirect evidence (i.e. studies on general populations which can be extrapolated to
interventions that are targeted toward migrants) was used. The GRADE method chosen to develop this guidance
states that indirect population or intervention evidence is justified when serious concerns exist, but indirect
evidence must be downgraded (63)
. Where evidence from non-migrant populations was used, input from the
expert panel regarding the applicability and validity for migrant populations was sought, and the indirectness of the
evidence was reflected in the evidence grade.
Table 1. Eligibility criteria used for all diseases
PICO and study characteristics inclusion criteria
Population
Migrant-specific studies used when available. Studies of any population (e.g. children and adults) that are considered
relevant, even if not migrant-specific.
Interventions
Screening, treatment and vaccine prevention interventions and programmes for the selected diseases are evaluated.
Comparisons
No screening or comparison of prevention interventions and/or programmes.
Outcomes
Reduction in morbidity or mortality, including surrogate outcomes or disease transmission.
Study characteristics
Design: systematic reviews, defined as a review with selection criteria, and search of at least one database.
As is often the case with evidence-based prevention guidelines, there is a limited number of primary studies that
assess clinical outcomes for screening versus no screening of certain conditions. For this reason, analytic
frameworks to identify key steps related to evidence of effectiveness along the screening-intervention pathway
were developed (all frameworks are published in the systematic reviews underpinning this guidance, see Section
1.3]. This approach guided the formulation of search strategies and identification of relevant literature for each
critical step along the screening evidence chain. Search terms and strategies appropriate for each infectious
disease were used to search for published literature in PubMed, the Cochrane Database of Systematic Reviews, and
Embase (January 2005 to May 2016) and updated where needed up to 2018. In addition, grey literature was
sourced via Google, as well as the US Centers for Disease Control and Prevention (CDC), ECDC, UNAIDS and WHO
websites. No language restrictions were applied for initial searches; certain review groups restricted language to
key European languages for feasibility.
Evidence was considered using a hierarchical approach, whereby meta-analyses, systematic reviews, and evidence-
based guidelines were given the most weight, followed by individual randomised controlled trials (RCTs), quasi-
experimental studies, observational studies and, lastly, expert opinion. The approach sought to build on existing
high-quality evidence. Additional evidence reviews were conducted if gaps were noted in the evidence base.
Two independent team members manually reviewed titles, abstracts and full text of identified citations, selected
evidence for inclusion, and compiled evidence reviews and PRISMA flow diagrams in accordance with PRISMA
guidelines (64). The methodological quality of included systematic reviews was assessed using AMSTAR (65)
and/or individual observational studies using the Newcastle Ottawa scales (66). For each cost-effectiveness study,
we extracted data for three specific questions: the size of the resource requirements, the certainty of evidence
around resource requirements, and whether the cost-effectiveness results favoured the intervention (67). Finally,
the certainty of economic evidence in each study (using the relevant items from the 1997 Drummond checklist)
was assessed (68). Tables were created that showed characteristics of included studies, rated the certainty of the
effects for pre-selected outcome measures and created GRADE evidence profiles. The systematic reviews that
underpin this guidance were done in line with PRISMA reporting guidelines (64) and can be found in the published
systematic reviews as outlined in Section 1.3 as well as in the online supplementary material for this guidance,
which is available on request.

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
11
In addition, a systematic review of qualitative outcomes was conducted to study acceptability and accessibility to
screening and vaccination interventions, and to explore how migrants value such interventions (24). A team of
experts used the Health Beliefs Model and graded the key findings using the GRADE CERQual method. Results are
reported as implementation considerations in the sections of this guidance pertaining to each disease (69).
3.5 GRADE approach to develop evidence statements
Evidence-based statements were developed and graded using the GRADE tool (67) through an iterative evidence
consensus process. The review teams developed initial draft evidence-based statements using an evidence-to-
decision approach and assigned initial GRADE evidence ratings, which were then revised in consultation with the ad
hoc scientific panel.
An initial step was using the GRADE approach to rate the certainty of evidence starting with a simplified
categorisation of study types (i.e. meta-analyses and RCTs, observational studies and expert opinion). The rating
scheme allows for factors that would raise or lower a level of certainty. Factors that would lower certainty of
evidence include risk of bias, inconsistency across the RCTs, indirectness and publication bias; factors that would
increase certainty of evidence include large effect size and an observed dose–response effect.
The certainty of evidence rating reflects the extent to which our confidence in an estimate of the effect is adequate
to support a particular option. Evidence was graded as high, moderate, low or very low certainty, based on how
likely further research is to change our confidence in the estimate of effect (Table 2). Low certainty and very low
certainty do not mean absence of evidence for effectiveness, but rather signal potential need for more research to
improve the precision of the estimate of effect.
Table 2.
Interpretation of GRADE certainty of evidence
High
We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate
We are moderately confident in the effect estimate. The true effect is likely to be close to the estimate of
the effect, but there is a possibility that it is substantially different.
Low
Our confidence in the effect estimate is limited. The true effect may be substantially different from the
estimate of the effect.
Very low
We have very little confidence in the effect estimate. The true effect is likely to be substantially different
from the estimate of effect.
We used the GRADE evidence-to-decision approach (67) to frame evidence and develop statements, and ultimately
rate the strength of the evidence-based statements. With input from the ad hoc scientific panel, agreement was
made to define, assess and report vaccination and screening evidence on the following 11 GRADE evidence-to-
decision criteria:
• Is the problem a priority? Assess the burden of infectious diseases in migrant populations and current
approaches in the EU/EEA.
• What are the desirable and undesirable effects of the intervention?
• What is the certainty of evidence?
• Values: is there important uncertainty about or variability in how much people value the main outcomes?
• Balance of effects: does the balance between desirable and undesirable effects favour the intervention?
• Resources required: how large are the resource requirements (costs)?
• Certainty of evidence of resource requirements.
• Cost-effectiveness: does the cost-effectiveness of the intervention favour the intervention?
• Equity: What could be the impact on health equity?
• Acceptability: Is the intervention acceptable to key stakeholders?
• Feasibility: Is the intervention feasible to implement?
The evidence from the quantitative evidence reviews and qualitative synthesis was put into GRADE Pro (70) to
facilitate presentation of these criteria and draft evidence-based statements (67). Evidence-to-decision criteria
state that the larger the difference between the desirable and undesirable effects, the higher the likelihood that a
strong option is warranted. The narrower the difference, the higher the likelihood that a weak or conditional option
is warranted. The higher the certainty of evidence, the higher the likelihood that a strong option is warranted.
When an intervention improves health equity a stronger option may be warranted. The more values and
preferences vary, or the greater the uncertainty in values and preferences, the higher the likelihood that a weak or
conditional option is warranted. Table 3 outlines the definitions of the GRADE strength of evidence-based
statements.

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
12
Table 3. Interpretation of GRADE strength of recommendation
Strong recommendations
Those in which we are confident that the desirable effects of an intervention outweigh its undesirable
effects (strong option for an intervention) or that the undesirable effects of an intervention outweigh its
desirable effects (strong option against an intervention). They imply that most individuals will be best
served by the recommended course of action and that the recommendation can be adopted in practice
or as policy in most situations.
Conditional
recommendations
Those for which the desirable effects probably outweigh the undesirable effects (conditional option for
an intervention) or undesirable effects probably outweigh the desirable effects (conditional option
against an intervention), but appreciable uncertainty exists. Conditional statements imply that most
people would want the recommended course of action, but that some would not. For clinicians, this
means that they must recognise that different choices will be appropriate for each individual, and that
they must help each person arrive at a management decision consistent with his/her values and
preferences. Policy making will require substantial debate and involvement of various stakeholders.
3.6 FACE survey
The ad hoc scientific panel members completed a FACE survey (feasibility, acceptability, cost and equity). The FACE
survey is designed to assess perceptions of: 1) the level of priority for the problem being addressed and 2) barriers
or enablers related to the evidence-based statements’ feasibility, acceptability, cost, and health equity. The findings
from the survey have been incorporated into each disease section in this guidance.
Panel members were presented with 13 screening and vaccination evidence-based statements for the key
infectious diseases and asked to rate implementation priorities for each disease under consideration (very low, low,
moderate, high). They were then asked to indicate the level of feasibility, acceptability, cost (resource use) and
equity for each option based on the FACE constructs (Table 4).
Table 4. Constructs of the FACE survey
Constructs
FACE questions
Feasibility
Would the option be sustainable? Would there be important barriers that are likely to limit the feasibility of
implementing the option?
Acceptability
Do you feel the option would be acceptable to stakeholders (including your organisation)?
Cost (resource use)
Would the current costs of the intervention be large?
Health Equity
Do you feel the option would positively impact health equity compared to current status? Are there groups or
settings (taking into account burden, access and treatment) that might be disadvantaged in relation to the
option considered?
3.7 Evidence review process and guideline development
The evidence review and guideline development process consisted of the following steps.
First, the evidence synthesis reviews were circulated to the full ECDC advisory group (consisting of the ad hoc
scientific panel, other experts, and observers) to assess and provide feedback on proposed evidence-based
statements for intervention.
Second, a video conference meeting was held on 8 May 2017 during which the ad hoc scientific panel was
presented with the preliminary findings of the evidence reviews for each disease and given the option to provide
feedback on the evidence-based statements. The scientific panel then used the GRADE Panel Voice Software (18)
to review and vote on all criteria of the evidence-to-decision summaries. Panel Voice allows each panel member to
enter a judgment on the evidence and provide narrative comments. FACE categories were classified by the panel’s
level of agreement as follows: high agreement (>75% of ad hoc panel), medium/moderate agreement (50–75%),
and low agreement (<50%). Differences in opinion or interpretation with regard to the guideline statements or the
evidence review were resolved through facilitated discussions in teleconferences or direct communication.
Third, the guidance document was developed and circulated to the full advisory group in order to assess the
evidence statements for intervention. Following revisions, a draft of the final guidance was sent to the ad hoc
scientific panel and ECDC disease leads for final review prior to publication.

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
13
4. Conclusions
This chapter outlines the evidence and key areas to be taken into consideration when designing and implementing
screening and vaccination programmes for key infectious diseases for newly arrived migrants in the EU/EEA. It
represents a synthesis of the systematic reviews and input from the ad hoc scientific panel and the advisory group.
The conclusions are presented for active TB, LTBI, HIV, hepatitis B, hepatitis C, schistosomiasis and
strongyloidiasis, and VPDs, with each section following a similar structure:
• Burden of disease
• Summary of evidence, focusing on effectiveness and cost-effectiveness
• Implementation considerations
• Ad hoc scientific panel opinion
• ECDC assessment
• Evidence gaps and future research needs
• Recommendations from other national and international guidelines
Summary tables provide an overview of the evidence that informed the evidence-based statements for each
disease area, with each table presenting:
• Data from publications included in the evidence review, on which conclusions have been based, under the
headings of ‘effectiveness’ and ‘cost-effectiveness’
• Strength of the body of evidence from the evidence review: certainty of evidence (GRADE)
• FACE survey results
• Strength of the recommendations
• Implementation considerations
The characteristics of included studies for effectiveness and cost-effectiveness, PRISMA flow diagrams for included
studies, and the GRADE profile tables specifying the certainty of evidence for each disease are available on the
ECDC website.

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
14
4.1 Active tuberculosis
Burden of disease
TB is a public health priority in the EU/EEA, and countries have committed themselves to the WHO End TB Strategy
and its goal of eliminating the global TB epidemic and targets of reducing TB deaths by 95%, cutting new cases by
90% between 2015 and 2035, and ensuring that no family is burdened with catastrophic expenses due to TB (71-
73, 74 ).
The foreign-born population makes up a considerable and increasing number and proportion of all TB cases in
EU/EEA countries with low TB incidence (< 10 cases/100 000 population), and this is a challenge for TB elimination
efforts in the EU/EEA (72, 74). Between 2007 and 2016, the proportion of reported TB cases in the foreign-born
population in the EU/EEA increased from 13.6% to 32.7% (75, 76). There are wide variations across the region: in
many low-TB-incidence EU/EEA countries, more than half of all TB cases occur among foreign-born individuals (74)
but in EU/EEA countries with a higher TB incidence they make up a minority of cases. A considerable proportion of
internal and external migrants within the EU/EEA were born in countries with a high TB incidence (Figure 2].
Figure 2. WHO global map of TB incidence
* Source: Global tuberculosis report 2017. Geneva: World Health Organization; 2017. Licence: CC BY-NCSA 3.0 IGO. Reproduced
with permission.
Summary of evidence
Given the disproportionate TB case notifications in migrant populations and increasing TB rates in the EU/EEA,
enhanced TB control strategies among migrants will be necessary to achieve TB elimination in the EU/EEA (defined
as achieving a rate of less than one case of TB per 1 000 000 population) (77, 78). There are two main approaches
to TB control among migrants:
• Identification of active TB with a chest radiograph (CXR) before or soon after arrival in the host country to
detect prevalent active TB cases to limit onward transmission. Many low-TB-incidence EU/EEA countries
screen migrants for active TB on, or soon after, arrival (79). The migrant groups targeted for screening and
the location of screening are different for each country (80, 81).
• Identifying and treating LTBI in migrants from high-TB-burden countries to prevent TB reactivation (80).
Effectiveness
We developed an analytic framework (19) and included six systematic reviews and one ECDC report that addressed the
key questions along the evidence chain for screening for active TB among migrants. These included three systematic
reviews on the yield of active TB screening in migrants (82-84), two systematic reviews on the performance of CXR to
detect active TB (85, 86), one systematic review on the acceptability of CXR screening (87), and one ECDC report on TB
treatment outcomes in Europe among those born in (or outside) the EU/EEA (75 ).
Three systematic reviews assessed the yield of detecting active TB among migrant populations in CXR screening
programmes performed prior to and after arrival in the EU/EEA and other low-TB-incidence countries (82-84). The yield
of active TB was heterogeneous across studies and varied by migrant type, timing of screening (before/after arrival) and
the setting in which the screening was done, but was consistently higher with higher TB incidence in the country of

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
15
origin. Klinkenberg et al. found that the overall yield of active TB screening programmes in migrants upon and after
arrival in 26 studies done in EU/EEA countries was 350/100 000 population (82). The yield differed by migrant type
(asylum seekers: median 350/100 000, (interquartile range (IQR): 250-410) and other migrants: 170 [100-630]) and by
the setting where the screening was conducted (port of arrival: 360 (IQR: 100-5,200); reception/holding centres: 290
(IQR: 100-380); community post arrival: 220 (IQR: 100-380); and occasional screening: 1 720 (IQR: 730-2,740)).
Arshad et al. assessed the yield of active TB screening among migrants originating from intermediate- or high-TB-
incidence countries upon and after entry to low-TB-incidence countries and also found a similar overall yield of active TB
case detection of 349/100 000 population. The yield also varied by migrant type (refugees: 1 192 (95% confidence
interval (CI): 668-1 717); regular migrants: 284 (95% CI: 204-364) and asylum seekers: 270 (95% CI: 198-342)) and
TB incidence in the country of origin (Europe: 236 (95% CI: 131-340); Africa: 655 (95% CI: 319-990); and Asia: 1 117
(95% CI: 625-1 608)) (83). Finally, Aldridge et al. assessed the yield of CXR screening for active TB among migrants in
the pre-entry TB screening programmes, a compulsory part of the immigration process with higher coverage than upon-
or after-entry programmes (84). No overall estimates were presented, but the yield increased steadily with the TB
incidence in migrant country of origin. The yield was 19.6/100 000 in migrants originating from countries with a TB
incidence of <50/100 000 and 336/100 000 in migrants originating from countries with a TB incidence greater than
350/100 000 (84).
Two systematic reviews addressed the performance of CXR to detect active TB in those >15 years of age. CXR is highly
sensitive (98%) and moderately specific (75%) to detect active TB in the presence of any abnormality compatible with TB
(85, 86, 88). Screening for TB symptoms is less reliable, with moderate sensitivity (70%) and specificity (61%) (85, 86).
An ECDC report found that TB treatment outcomes were similar or better in those born outside compared with those
born inside the EU/EEA (75). More specifically, treatment success was as high in those born outside the EU/EEA (for all
regions of origin) compared with those born in the EU/EEA [77.4% vs 74.6%), but their failure rates (0.2% vs 2.4%) and
default rates (5.4% to 6.6%) were lower (75). Mitchell et al. conducted a review to determine the acceptability of
targeted TB screening and active case finding among vulnerable and at-risk groups and found that TB screening was well
accepted by the majority of risk groups, including migrants (85% range (55%-96%)). Lower acceptability was found
among persons living with HIV/AIDS and individuals in refugee camps and internally displaced persons (87).
Cost-effectiveness
There are very little data on the cost-effectiveness of active TB screening in migrant populations as only three
individual studies were identified (89-91). These studies showed a clear benefit of screening with CXR among high-
prevalence groups, close contacts of those with known TB, and migrants at entry if they originate from
intermediate- or high-TB-incidence countries (defined as >60/100 000 and >120/100 000, respectively) (89-91).
These studies demonstrated that increased cost-effectiveness was associated with higher TB incidence in the
country of origin, which suggests that programmes will be more cost-effective when targeting migrants from
countries of origin with a high incidence TB.
Implementation considerations
Migrants, particularly refugees, asylum seekers, and undocumented migrants, may be underserved and face a
range of socio-economic, cultural and linguistic barriers to accessing healthcare and treatment in the EU/EEA as
well as a lack of rights to free healthcare (92). Other barriers include low perception of risk, disease-related stigma,
and fear of discrimination by health services (93). Although uptake of TB screening is often high in migrants, those
without regular status may avoid voluntary screening programmes (33, 87); migrants may also face barriers to
follow-up care and treatment. Adherence to active TB therapy may be challenging for some vulnerable migrants as
it requires a minimum of six months of treatment and close follow-up to monitor for drug toxicity (94, 95).
Adherence to TB therapy among migrant populations may be enhanced by engaging non-clinical professionals who
can coordinate TB care, providing reminders for clinic visits and through addressing language and cultural barriers
(96-101). Front-line healthcare professionals and policymakers will need to understand and address healthcare
barriers experienced by migrants to ensure uptake and completion of active TB screening and treatment.
Active screening programmes are limited by the fact that they do not capture or prevent the majority of incident TB
cases occurring in the EU/EEA, which occur primarily due to reactivation of LTBI or new acquisition during travel
(79, 80). Most TB screening programmes in Europe target asylum seekers and refugees and therefore miss other
circulating migrant groups. Coverage is low, and the focus is around on-arrival screening, despite the fact that the
risk remains high for several years after arrival (93). Pre-entry CXRs may not cover the majority of migrants in
countries such as Italy or Greece, where many arrive through irregular routes. A minimum package of services for
TB prevention, diagnosis, treatment, and care for migrants and refugees in the WHO European Region has recently
been outlined, which highlights the importance of targeted, culturally sensitive and accessible services, of reducing
stigma, and of cross-border collaboration on TB screening and care across the entire migration trajectory (57).
Screening programmes for active TB in migrants will need to be tailored to the local TB epidemiology and health
system context in host countries (72, 73). Programmes will also need to be adapted to the unique legal, social, and
cultural needs of migrant populations, involve migrants in their set-up and delivery, alongside tailored awareness-
raising about the benefits of early screening within migrant communities (93).

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
16
Ad hoc scientific panel opinion
The ad hoc scientific panel members were in agreement that active TB case finding in migrant populations is an
important TB control strategy as it allows for early detection and treatment, reduces individual morbidity, and
prevents onward TB transmission. The panel concluded that the strength of the recommendation was conditional
on the prevalence of TB in a migrant’s country of origin, and the focus should be on screening migrants from
intermediate- to high-TB-incidence countries.
The ad hoc scientific panel were asked for their opinion on the evidence relating to: feasibility, acceptability, cost
(resource use), and equity of active TB screening among migrants: high level of agreement (>75% of scientific
panel), medium level of agreement (50–75% of scientific panel), and low level of agreement (<50% of scientific
panel). The results of the FACE survey were as follows:
• High level of agreement (87%) that active TB screening among migrants is a priority in the EU/EEA.
• Medium level of agreement (64%) that active TB screening among migrants is feasible in the EU/EEA.
• Medium level of agreement (71%) that active TB screening among migrants is acceptable in the EU/EEA.
• High level of agreement (79%) that active TB screening among migrants is equitable in the EU/EEA.
The scientific panel agreed that evidence was very low to moderate quality across all key questions. They also
agreed that there were additional considerations to be taken into account when offering screening to migrants for
active TB. Healthcare accessibility was considered by all to be a critical issue when designing migrant screening
programmes. Programmes need to address the barriers that migrants face in accessing healthcare, including lack
of entitlement to free statutory health services, in order to ensure high uptake of screening and linkage to care and
TB treatment. Screening migrants increases the complexity of national TB programmes because language and
cultural issues will need to be addressed and resourced.
ECDC assessment
Active TB case finding in at-risk populations is an important TB control strategy as it allows for early detection and
treatment, reduces individual morbidity and mortality, and prevents TB spread to others. The CXR is a highly
sensitive and moderately specific test to detect active TB. The yield of active TB screening among migrants and the
associated cost-effectiveness consistently increases with increasing TB incidence in the country of origin. Screening
uptake and treatment completion, however, may be difficult among vulnerable migrants due to barriers to
accessing and remaining in healthcare. Furthermore, active TB screening is limited by the fact that it only captures
or prevents a minority of migrant TB cases in the EU/EEA, as most result from reactivation of latent infection after
arrival. Significant data gaps limit the ability to confidently prioritise TB control efforts for this population. Despite
these limitations and data gaps, the benefits of active TB screening likely outweigh the harms and costs if targeted
among migrants originating from high-TB-incidence countries. The optimal threshold of incidence in countries of
origin at which to screen is yet to be defined.
Evidence-based statement
Offer active TB screening using chest X-ray (CXR) soon after arrival for migrant populations from high-TB-
incidence countries. Those with an abnormal CXR should be referred for assessment of active TB and have a
sputum culture for Mycobacterium tuberculosis.
(Certainty of evidence: low)

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
17
Table 5. Evidence synthesis and guidance for active TB screening in migrants
Effectiveness
Cost-effectiveness
Certainty
of evidence
(GRADE)
FACE survey*
Strength of
recommendation
Implementation
considerations
The yield of active TB
detected through CXR
screening of migrants was
heterogeneous across studies
and varied by migrant type
and the setting in which the
screening was done, but
consistently increased with
higher TB incidence in a
screened migrants’ country of
origin (82-84).
CXR is highly sensitive to
detect active TB but to
increase specificity must be
confirmed with a culture for
TB. Presence of symptoms is
insufficiently sensitive or
specific to detect active TB
(85, 86, 88).
Active TB treatment is highly
effective but adverse events
occur in a significant number
making close follow-up
during therapy critical (75).
The optimal threshold of
incidence in countries of
origin at which to screen is
yet to be defined (89-91).
There is very little
data on the cost-
effectiveness of
active TB screening
in migrant
populations.
Increased cost-
effectiveness was
associated with
higher TB incidence
in the country of
origin, which
suggests that
programmes are
more cost-effective
when targeting
migrants from
intermediate and
high-incidence TB
countries of origin
(89-91).
Low
The ad hoc scientific
panel rated
active TB
screening among
migrants in the
EU/EEA as follows:
• High priority
• Moderate
agreement on
acceptability
• Moderate
agreement on
feasibility
• High agreement
on equitability.
Conditional
recommendation,
based on country of
origin (intermediate-
to high-incidence
country of origin).
Migrants face
numerous barriers to
accessing healthcare
including socio-
economic, stigma,
linguistic and cultural
and lack of regular
status and insurance
that may decrease
uptake of TB
screening and/or
treatment.
Programmes should
address these
barriers to ensure
high uptake of
screening and
linkage to care and
TB treatment.
* FACE categories were classified by the level of agreement of the panel as follows: high (>75% of ad hoc panel), medium (50–
75%), and low (<50%).
Evidence gaps and future research needs
Designing highly effective active TB screening programmes requires robust population-based studies on the yield of
active TB screening among migrants by age group, data on migration type, determining both the timing of screening and
the optimal threshold of incidence in countries where screenings will be conducted, and data on associated cost-
effectiveness. Additional studies that determine the absolute and attributable impact of active TB programmes on TB
control in low-incidence EU/EEA countries and estimates of adherence to follow-up care and treatment are needed.
Finally, evidence on the comparative effectiveness and cost-effectiveness of different TB control strategies (active vs. LTBI
screening) for migrants are required to prioritise TB control efforts for this population.

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
18
Recommendations from other national and international guidelines
Table 6. Active TB screening recommendations for migrants in selected low-TB-incidence countries
Country
When, how and who to test
Australia (102-
104)
Pre-entry CXR screening required for permanent or provisional visa applicants and some categories of temporary visa
applicants (intended duration of stay of ≥ 6 months; healthcare professionals and trainees and child care workers and
trainees) if originating from a high-TB-risk country
Age-specific requirements:
• < 2 years – history and physical examination; if positive → CXR
• 2–10 years – history and physical examination + TST or IGRA if coming from a higher TB burden country (not
quantified); if positive → CXR
• 11 years and above – history and physical examination + CXR
• If CXR is suggestive of TB or there are signs and symptoms of pulmonary TB
→
sputum microscopy and cultures.
Canada (105-
108)
Pre-entry screening required for permanent visa applicants and some categories of temporary visa applicants (intended
duration of stay of ≥ 6 months) and certain professional groups and applicants; also required for extended visitors’
visas (‘parents and grandparents super visa’) for those coming from a high TB-risk country (defined as a 3-year averag
e
TB incidence of >30/100 000 cases of TB).
Age-specific requirements:
• 0–10 years – history and physical examination; if positive → CXR
• 11 years and above – history and physical examination + CXR
• If CXR is suggestive of TB or there are signs and symptoms of pulmonary TB → sputum microscopy and cultures.
France (109)
For all recently arrived migrants, within four months of arrival, a medical visit is recommended that includes tuberculosis
screening for migrants arriving from high incidence countries (>40 /100 000].*
*
An update of current TBI recommendations in France is underway.
Ireland (8)
Post-arrival CXR screening for all migrants from countries with incidence ≥40 cases per 100 000 population
Age-specific requirement:
• <16 years or pregnant: TST, unless medical examination → CXR + sputum examination
• ≥16 years: CXR
• 16–35 years of age from sub-Saharan Africa or country incidence >500/100 000: CXR +TST
• If CXR is suggestive of TB or if there are signs and symptoms of pulmonary TB
→
sputum microscopy and cultures
Italy (13)
The search of active TB diseases should be part of the initial medical assessment of migrants and for all during the
reception process.
Migrants should be made aware of TB symptoms and should be encouraged to report them.
Migrants with cough lasting for more than two weeks should undergo CXRsor – if not available immediately –
molecular
rapid test to ensure detection and isolation of contagious cases.
TST and IGRA are not recommended for the diagnosis of active TB disease.
Routine CXR is not recommended in asymptomatic subjects.
If TB disease is confirmed, complete care is to be assured, including immediate and free access to treatment and
continuity of cure if the patients moves to other reception centres or countries.
UK (110-112)
Pre-entry screening is required for the migrants who intend to stay in the UK for six months or longer and who come
from countries with higher TB burden (not quantified, but list of countries provided).
Category-specific requirements:
• Children below 11 years: symptom screen; if positive → CXR
• Applicants of 11 years and above: symptom screen + CXR
• Pregnant women: may choose to be screened with 1) symptom screen + CXR with double shielding, 2) symptom
screen + sputum microscopy and cultures or 3) postpone the CXR and TB clearance until after delivery.
• If CXR is suggestive of TB or there are signs and symptoms of pulmonary TB
→
sputum microscopy and cultures.
US (113)
Pre-entry CXR screening is required for immigrant visa applicants, refugees and asylum seekers.
Age-specific requirements:
• < 2 years – history and physical examination; if positive → CXR
• 2–14 years – history and physical examination + TST or IGRA if coming from a country with a TB incidence o
f
≥
20/100 000; if positive → CXR
• 15 years and above – history and physical examination + CXR
• If CXR is suggestive of TB or there are signs and symptoms of pulmonary TB
→
sputum microscopy and culture.
CXR = chest X-ray; TB = tuberculosis; TST = tuberculin skin test; IGRA = interferon gamma release assays.

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
19
4.2 Latent tuberculosis infection
Burden of disease
TB control programmes in the EU/EEA have successfully managed to reduce TB rates by 50% over the past 20
years (72, 73, 76, 98). However, the rate of TB decline of 4.3% per year over the past decade (2007–2016) in the
region is insufficient to achieve the goal and targets of the WHO End TB Strategy (72, 73, 76, 98). It is projected
that a mean decline of 18% per year will be necessary to meet the WHO goal and that TB control strategies must
be scaled up, including addressing the burden of LTBI (72, 114, 115).
The majority of the active TB cases in migrants in the EU/EEA are due to reactivation of LTBI acquired in the
country of origin. In high-TB-burden countries of origin (Figure 2), 22–31% of the population may have LTBI (76,
116, 117). High rates of LTBI, and low treatment completion rates, have been identified in data from migrant
screening programmes across Europe (93).
Summary of evidence
WHO has only conditionally recommended LTBI screening among migrants living in low-TB-incidence countries
(<10 cases/100 000 population), owing to reservations about implementation and the low quality of evidence of
the effectiveness and cost-effectiveness of LTBI programmes in these settings (118). A recent WHO Regional Office
for Europe Health Evidence Synthesis Report states that there is evidence for the effectiveness of incorporating
screening for LTBI into screening programmes targeting migrants from countries of high TB incidence, but there
was a lack of consensus on cost-effectiveness and numerous issues regarding effective implementation (57). We
present results of a systematic review on the effectiveness and cost-effectiveness of screening for LTBI among
migrants to the EU/EEA.
Effectiveness
An analytic framework was developed (20) which included seven systematic reviews that addressed the LTBI
screening chain of evidence: three on the test properties of LTBI screening tests (119-121); two on the efficacy
and harms of LTBI treatments (122, 123); and two on the LTBI care cascade, including uptake of screening and
treatment initiation and completion (124, 125).
Three systematic reviews assessed the properties of the diagnostic tests used in LTBI screening in Bacillus
Calmette–Guérin) (BCG) unvaccinated populations. The tuberculin skin test (TST), at a 10 mm cut off, and
interferon-gamma release assays (IGRAs) were found to have similar and good sensitivity and high specificity to
detect LTBI (79% and >97%, receptively) (119, 121). TST is, however, limited by lower specificity (59%) in BCG-
vaccinated populations (119). Both tests poorly predicted the development of active TB. The positive predictive
value (PPV) and the pooled incidence rate ratios (IRR) estimated by comparing test-positive and test-negative
cohorts, for TST and IGRA, were similar (120). The PPV (range) and the IRR (95% CI) was 1–7% and 2.07 (1.38–
3.11) for the TST and 0–13% and 2.40 (1.26–4.60) for IGRAs, respectively (120).
Several different regimens to prevent the development of active TB, including rifampicin (RIF) alone or in
combination with isoniazid (INH) and INH alone for 6–12 months, are equivalent and have moderate efficacy.
Based on the evidence reviewed by the panel, the odds of developing active TB among those who took INH for
6 months compared with placebo was 0.64 (95% CI 0.48-0.83), and the odds of developing TB with the 3–4
months of RIF regimens compared with placebo was 0.41 (0.18-0.86) (122). Similar efficacy was found for the
following three different comparisons: RIF monotherapy for 3–4 months vs. INH for 6–9 months; RIF + INH for
3 months vs. INH for 6–9 months and weekly rifapentine (RFP) + INH for 3 months vs. INH for 9 months. The
comparative relative risks (RR) with 95% CI for these RIF combinations vs. INH were 0.81 (0.47 to 1.4), 1.08 (0.65
to 1.79) and 0.44 (0.18 to 1.07), respectively (123). RIF-based regimens were better tolerated with lower
hepatotoxicity RR (0.15, 95% CI 0.07-0.4) and had better adherence (82% vs 69%, RR 1.19 (95% CI 1.16-1.22))
(123).
The LTBI care cascade – including the uptake of screening and treatment, and initiation (23–97%) and completion
(7–86%) of therapy – varied widely among migrants (125). The review by Alsdurf et al. found that only 18.8% of
all those eligible for screening completed LTBI therapy, and that this was low for all groups, including migrants
(14.3%) (124). This was due to progressive losses at all stages of the care cascade; 71.9% (95% CI 71.8-72.0)
completed testing, 43.7% (95% CI 42.5-44.9) completed medical evaluation, 35.0% (95% CI 33.8-36.4) were
recommended treatment, and only 18.8% completed treatment (124).
Cost-effectiveness
We included 16 cost-effectiveness analyses studies; however, the designs and outcomes for these studies were
heterogeneous. These studies focused on comparisons between LTBI screening strategies (e.g. TST, IGRA or
sequential TST/IGRA), or, among high-risk groups, comparisons with other screening techniques such as CXR for
active TB, a combination of CXR/TST, or no screening. Eleven of 16 studies addressed an LTBI screening strategy
and included a migrant group, however only three studies were specifically about migrants in EU/EEA countries

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
20
(126-128). The cost-effectiveness of screening strategies was dependant on test characteristics, which tests were
being compared, the cost of tests, and whether the population was BCG vaccinated.
In four studies, screening with a single-step IGRA was less costly or more cost-effective relative to TST screening in
migrants to prevent incident TB (126, 127, 129, 130). Performing an IGRA in migrants 16–35 years of age
originating from countries with a TB incidence of >150/100 000 was the most cost-effective LTBI strategy, with an
incremental cost-effectiveness ratio (ICER) of approximately GBP 20 000 (EUR 24 000) to GBP 30 000 (EUR
36 000) per active TB case prevented (126, 127). For migrants older than 45 years, the intervention was unlikely to
be cost-effective, with an ICER for IGRAs vs. no screening between USD 103 000 and USD 283 000 per QALY
gained (EUR 86 000 – EUR 236 000/QALY) (130).
In three other studies, the optimal LTBI testing strategy varied in different high-risk populations (migrants or TB
contacts) and was influenced by true LTBI prevalence and prior BCG vaccination (91, 131, 132). In those with a
high likelihood of a true positive TST (LTBI prevalence >5%) and who were BCG vaccinated after infancy,
sequential TST/IGRA testing was preferred over single TST or IGRA (91, 131). When sequential TST-IGRA testing
was compared with no testing, the ICER was EUR 560 (EUR 580) per life year gained (YLG); for IGRA compared
with TST-IGRA, the ICER was EUR 730 (EUR 757)/YLG in the scenario when LTBI prevalence was >5%. This was
robust across a wide range of LTBI prevalence. In contacts of active TB cases, sequential TST-IGRA testing was
also more cost-effective compared with no screening or single-step TST, with an incremental cost per active case
prevented of GBP 37 699 (EUR 48 020) – GBP 37 206 (EUR 47 392) (132).
Implementation considerations
Migrants face barriers that can hinder treatment initiation and completion (125, 133-135), and this is particularly so
with LTBI. Preventive treatment will likely be less of a priority compared with other competing priorities for
migrants soon after arrival. Individual barriers include the stigma related to TB and its association with HIV,
language and difficulties navigating the healthcare system (133). Migrants without regular status may lack the right
to healthcare access in many EU/EEA countries (92). Strategies that may improve treatment completion among
migrants include reminders for clinic visits, nurse counselling and addressing linguistic and cultural barriers (99-
101, 136, 137). Provider barriers include inadequate knowledge of which migrants should be screened or managed,
and this requires education and training (133, 138). Addressing barriers at all levels and at each step of the care
cascade will be essential to ensure individual and public health benefits of LTBI programmes. Less than half of
EU/EEA countries have LTBI programmes for migrants, and there are numerous challenges to developing and
implementing new programmes (79, 81, 139). These include the heterogeneity of migrant populations and
subgroups affected by TB in EU/EEA countries and economic and operational considerations. LTBI screening
programmes will need to be tailored to the local TB epidemiology, TB risk in migrant subgroups, and economic and
healthcare capacity in in host countries (72, 73).
Ad hoc scientific panel opinion
The scientific panel members were in agreement that LTBI screening and treatment among migrant populations is
an important TB control strategy and is required to achieve the WHO goal of eliminating TB. The panel concluded
that the strength of the recommendation was conditional and that LTBI screening and treatment should focus on
migrants from high-TB-incidence countries.
The scientific panel members were asked for their opinion on the evidence relating to: feasibility, acceptability, cost
(resource use), and equity of LTBI screening among migrants. The results of the FACE survey showed:
• a high level of agreement (87%) that LBTI screening among migrants is a priority in the EU/EEA;
• a medium level of agreement (57%) that LTBI screening among migrants is feasible in the EU/EEA;
• a medium level of agreement (64%) that LTBI screening among migrants is acceptable in the EU/EEA; and
• a high level of agreement (86%) that LTBI screening among migrants is equitable in the EU/EEA.
The scientific panel agreed that the quality of the evidence was very low to moderate across all key questions.
There was, however, a high level of agreement that LTBI among migrants was a priority for the EU/EEA. Given the
challenges of acceptability and feasibility of implementing LTBI programmes, the panel agreed that screening and
treatment for LTBI would be better targeted at high-risk groups, such as migrants coming from intermediate
or
high TB endemic countries. For health equity reasons, LTBI screening should be offered to migrants. Some panel
members felt that investing in LTBI screening may detract from other health priorities where healthcare resources
are limited.

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
21
ECDC assessment
Migrants account for a large and growing proportion of TB cases in low-TB-incidence EU/EEA countries, and most
of these TB cases are due to reactivation of LTBI. Addressing LTBI among migrants will therefore be critical to
achieving TB elimination. Tests to detect LTBI (TST and IGRA) when positive poorly predict the risk of developing
active disease. All LTBI therapies are equivalent and have moderate efficacy, but RIF-based therapies may be
preferred due to lower hepatoxicity and higher completion rates. The LTBI care cascade is weak, and only a small
proportion of migrants eligible for screening complete treatment (124) due to barriers to accessing and remaining
in healthcare. Limited economic analyses suggest that the most cost-effective approach may be targeting young
migrants from high-TB-incidence countries. Significant data gaps limit the ability to confidently prioritise TB control
efforts for this population. Widespread implementation of LTBI screening and treatment programmes is constrained
by challenges including the heterogeneity of migrant populations at risk, and economic and operational
considerations. Despite this, migrant-focused LTBI screening programmes may be effective and cost-effective if
they are highly targeted and well implemented.
Table 7. Evidence synthesis and guidance for LTBI screening in migrants
Effectiveness
Cost-effectiveness
Certainty of
evidence
(GRADE)
FACE survey*
Strength of
recommendation
Implementation
considerations
TST and IGRA have
high sensitivity to
detect LTBI but when
positive, both poorly
predict the
development of active
TB (119-121).
All LTBI therapies have
low to moderate
efficacy; however,
RIF-based therapies
may be preferred due
to lower hepatoxicity
and higher completion
rates (122, 123).
The LTBI care cascade
is weak and only a
small proportion
(<15%) of migrants
eligible for screening
complete treatment
(124, 125).
Limited economic
analyses suggest
that the most cost-
effective approach
may be targeting
young migrants
(<35 years of age)
from high-TB-
incidence countries
(>150 cases/100 000
population) (126,
127, 129, 130).
Cost-effectiveness
increased with
increasing TB
incidence in the
country of origin.
Low
The ad hoc scientific
panel rated LTBI
screening among
migrants in the EU/EEA
as follows:
• High priority
• Moderate
agreement on
feasibility
• Moderate
agreement on
acceptability
• High agreement on
equitability
Conditional
recommendation
based on country of
origin (intermediate-
to high-TB-incidence
in country of origin)
Migrants face many
barriers to accessing
healthcare; these
socio-economic,
linguistic and
cultural
factors need
to be considered.
TB-related stigma in
migrant
communities is an
important
consideration.
Those with irregular
status may lack the
right to access to
healthcare.
Challenges to
widespread
implementation in
EU/EEA countries
include
heterogeneous TB
risk among migrants
and economic and
operational
considerations.
* FACE categories were classified by the level of agreement of the panel as follows: high (>75% of ad hoc panel), medium (50–
75%), and low (<50%).
Evidence gaps and future research needs
Better evidence is needed on the individual, combined and attributable population contribution of risk factors
leading to progression from LTBI to active TB in migrants. Intervention studies that determine how to improve the
identification of target populations and retain them in care, as well as cost-effectiveness studies that assess these
interventions, will be needed to develop the highest impact programmes. Ultimately, better diagnostic tests that
accurately predict those individuals who will develop active TB, shorter, better tolerated treatment courses, and
more effective interventions to promote adherence, will be needed to achieve TB elimination.
Evidence-based statement
Offer LTBI screening using a tuberculin skin test (TST) or an interferon-gamma release assay IGRA soon after
arrival for all migrant populations from high-TB-incidence countries and link to care and treatment where
indicated.

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
22
Recommendations from other national and international guidelines
Table 8. LTBI screening recommendations for migrants in selected low-TB-incidence countries
Country
When, how and who to test
Australia (9)
• ≤ 35 years of age: offer LTBI screening with TST (cut-off 10 mm) or IGRA
• <5 years of age, TST preferred, 2–10 years: might have already been performed pre-entry
• > 35 years of age: based on risk factors and state/territory requirements
Canada (105)
There are no routine post-arrival domestic LTBI screening programmes for immigrants in Canada but LTBI
screening is recommended for the following groups:
• Screen immigrants with TST from countries with high TB incidence (>30/100 000] if fibronodular
c
hanges on CXR (done during post landing surveillance).
• Screen all children and adolescents <20 years on arrival or soon after.
• Screen all refugees aged 20–50 years.
• Screen those with underlying medical comorbidities that increase the risk of reactivation.
France (140)
For all children under 15 years of age from high-incidence countries, screening by IDR for latent tuberculosis
(expert opinion).*
* An update of current LTBI recommendations in France is underway
Ireland (8)
≥16 years of age: initial screen with CXR (>40/100 000]
• Normal: perform TST if from sub-Saharan Africa or a high incidence country (>500/100 000]
• Abnormal: rule out active disease, offer LTBI treatment
<16 years of age or pregnant: TST (>40/100 000)
Italy (13)
• Offer TST (alternatively IGRA may be used, in particular if previously vaccinated) to all migrants from
high-TB-incidence countries (>100/100 000 inhabitants) who are expecting to stay for at least six
months
• Use TST screening test for children < 5 years.
• Subjects with positive TST (cut-off ≥10 mm, use the ≥5 mm cut-off if HIV-positive or severe
ly
m
alnourished) or IGRA tests should be offered CXR and other diagnostic tests.
• If active disease is excluded, subjects with positive TST or IGRA tests should be offered preventive
treatment.
UK (141)
Migrants who are between 16 and 35 years of age and have arrived in England within the previous five years
and were born or lived for more than six months in sub-Saharan Africa or countries where TB incidence is
≥150 per 100 000 population are offered LTBI screening and will be treated if positive.
US (142-144)
All newly arrived refugees are tested with TST or IGRA if not done pre-departure; if positive, treatment is
offered.
Other migrants: 2–14 years of age and originating from countries with a TB incidence of >20/100 000 are
offered a TST or IGRA in the pre-arrival setting; if positive, treatment is offered.
In the post-arrival setting, screening individuals that are likely to be infected with Mycobacterium tuberculosis
and have an intermediate or high risk of disease progression should be prioritised for LTBI screening and
treatment.
CXR = chest X-ray; LTBI = latent tuberculosis infection; TB = tuberculosis; TST: tuberculin skin test; IGRA: interferon-gamma
release assay.

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
23
4.3 HIV
Burden of disease
In the EU/EEA, 29 444 HIV diagnoses were reported in 2016 (145). An estimated 15% of people living with HIV
(n = 122 000) remain unaware of their HIV-positive status (146), limiting the accuracy of data on HIV prevalence
in the EU/EEA. Although the overall number of HIV diagnoses in migrants from countries where HIV is prevalent
has declined in the EU/EEA over the past decade, migrants still account for 40% of reported cases (17% from sub-
Saharan African countries and 23% from other countries) (145). In 2016, foreign-born cases ranged from <1% of
all new HIV diagnoses (Poland, Romania) to >70% of new HIV diagnoses (Ireland, Malta, Sweden) (145). Some
migrant groups have a higher frequency of delayed HIV diagnosis associated with high levels of HIV stigma (147,
148), and some subgroups of migrants may participate in high-risk behaviour for HIV, such as multiple sexual
partners, low and inconsistent condom use, high alcohol consumption, and drug use (148). While some migrants
may acquire HIV in their country of origin (Figure 3), new data suggest that more than half of new infections
among migrants occur after their arrival in EU/EEA host countries (104, 149-152).
Figure 3. UNAIDS global map of HIV prevalence
* Source: UNAIDS Report 2016. Geneva: 2016.Reproduced with permission from UNAIDS
Summary of evidence
HIV testing in at-risk populations, including migrants from communities with high (>1%) HIV prevalence, migrant
men who have sex with men, migrants who inject drugs, and migrants who sell sex, is an important HIV control
strategy as it allows for early detection and treatment, reduces individual morbidity and mortality, and prevents
onward transmission. HIV testing is highly accurate, and rapid testing strategies demonstrate acceptability and
cost-effectiveness. Limited access to healthcare and HIV-related stigma pose significant barriers to testing uptake
and treatment (148, 153).
In WHO’s consolidated HIV testing guidelines (2017), WHO recommends community-based HIV testing services
(with linkage to prevention, treatment and care services) for key populations (including migrants, refugees and
displaced populations), in addition to provider-initiated testing and counselling (154). Similarly, ECDC has
recommended that testing be offered to migrants from high-prevalence countries with clear referral pathways to
treatment; testing should include undocumented migrants and migrants of uncertain residency status (155). Most
EU/EEA countries report having national guidance on HIV testing (102, 156), and at least 22 countries
acknowledge that migrants are vulnerable to HIV infection, but six of these countries do not explicitly recommend
HIV testing for migrants (157). Currently, there are no EU/EEA-wide HIV testing guidelines or strategies specifically
tailored for migrant populations, and questions regarding implementation of such programmes remain.
Effectiveness
As stated above (Section 3.4), studies on high-risk migrant groups were prioritised. However, when migrant-specific
studies were lacking, indirect evidence [i.e. studies on general populations which can be extrapolated to
interventions that are targeted toward migrants) was used. Where evidence from non-migrant populations was

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
24
used, input from the expert panel regarding the applicability and validity for migrant populations was sought, and
the indirectness of the evidence was reflected in the evidence grade.
Using the analytic framework for the systematic review (21), four systematic reviews were identified relating to
voluntary testing for HIV (150, 158-160) that reported on outcomes. One review studied rapid testing versus
conventional testing
7
in populations at high risk for HIV (150), one examined universal versus selective testing
(160), another considered provider-initiated testing versus conventional testing (158), and another looked at
telephone outreach testing approaches (159). None of the reviews reported on post-test counselling strategies,
linkage to care, or clinical outcomes.
A systematic review conducted by the US Agency for Healthcare Research and Quality reported that HIV testing
was accurate (rapid test >90% sensitive, Western blot and ELISA >99% sensitive (160). However, the review
found that targeted screening programmes that only test patients with identified risk factors may still miss a
proportion of cases (160). The majority of included RCTs studied populations with intermediate (≥0.1%) or high
HIV prevalence (≥1%). One RCT, from the USA, studied migrants (161). One meta-analysis reported that providing
rapid voluntary testing improved testing uptake and receipt of results in comparison to conventional testing (RR =
2.95, 95% CI: 1.69-5.16) (150). Finally, one RCT showed repeat testing was more likely among individuals
receiving community-based rapid testing
(RR = 2.28, 95% CI 0.35 to 15.07) (150).
Evidence indicates that treatment reduces the risk of AIDS-defining events and mortality in persons with less
advanced immunodeficiency and reduces sexual transmission in discordant couples (162-165). The US review
reports universal opt-out rapid testing is associated with higher likelihood of testing compared with physician-
directed, targeted rapid testing (160). Universal testing was also associated with a higher median CD4 count and
lower likelihood of CD4 count <200 cells/mm
3
at the time of diagnosis compared with targeted HIV testing, but
these differences were not statistically significant (160).
Cost-effectiveness
There is very little data on the cost-effectiveness of HIV testing in migrant populations. We identified eight studies on the cost-
effectiveness of, and resources required for, HIV testing and care (166-173). Three studies commented on HIV testing strategies
(170-172). The economic evidence suggests that rapid testing is likely to be preferable to conventional testing across a range of
contexts, largely due to the ability to more effectively integrate testing and counselling. One study supports the use of a single
rapid test (168), while another suggests possible cost savings with multiple rapid assays (170).
Evidence supporting multiple rapid
tests, rather than a single rapid test followed by later confirmatory test if positive, is mixed.
In low prevalence settings (<0.1%),
a single rapid assay is also likely to be cost effective.
Implementation considerations
People living with undiagnosed HIV infection, and those diagnosed with HIV but not yet on treatment, contribute
disproportionately to the number of new HIV infections (174). Uptake by migrants in EU/EEA screening
programmes for HIV was found to be high (median 82.46% (range 77.06-96.77)) (167), suggesting that migrants
may be proactive about screening. Screening needs to be provided in a culturally appropriate environment and
efforts should be made to reduce stigma around disease screening, with more emphasis placed on tackling late
presentation among migrants (175). More than half of EU/EEA countries do not provide antiretroviral therapy (ART)
free of charge for undocumented migrants (176) – which will undoubtedly impact on other vulnerable migrants –
reducing the likelihood that these individuals will come forward for testing. Barriers to testing include perception of
low risk, fear and stigma of the disease, fear of disclosure, discrimination, financial limitations, poor access to care,
and lack of knowledge about where to obtain testing, and lack of entitlement to medical care due to migration
status (104, 177, 178). There were low levels of HIV knowledge among certain migrants (177, 178). The most
consistent benefit of testing was reassurance of negative status (177). Stigma is an overarching barrier to
screening and treatment (177), as is fear that a positive test result may have a negative impact on immigration
status or refugee claim (177, 179). ECDC guidance on antenatal screening for infections indicates several
approaches for increasing the uptake of antenatal screening among migrant women such as offering appropriate
assistance to lower communication barriers (by taking into account language, literacy levels, or individual or
cultural specifics) and facilitate access to antenatal care through outreach services and informal networks (180).
7
Rapid voluntary counselling and testing (VCT) refers to voluntary enrolment where results are obtained within 24 hours and
includes outreach counselling, results delivery and treatment options. Conventional testing for HIV is defined as traditional
laboratory testing techniques for HIV in health care settings where patients have to wait for more than 1 day to receive their
results. HIV testing is accurate (Rapid Test >90%, Western Blot and ELISA >99%).

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
25
Ad hoc scientific panel opinion
The scientific panel were in agreement that offering voluntary HIV testing in migrant populations is an important
HIV control strategy, and a human right, as it allows for early detection, treatment and prevention of transmission.
The panel concluded that the strength of the recommendation was conditional on the prevalence of HIV in the
migrants’ country of origin or local regions in the EU/EEA. Voluntary HIV screening, either rapid testing or
conventional testing, should focus on testing and treating migrants coming from countries with an HIV prevalence
rate of ≥1% or migrants belonging to populations at high risk for HIV acquisition (i.e. men who have sex with
men, people who inject drugs, and people who sell sex). Addressing late presentation in migrant populations and
transmission after arrival was also considered a critical objective of HIV screening programmes targeting this
group. Importantly, the scientific panel were in agreement that any screening initiatives need to be accompanied
by access to follow-up treatment and care, provided free of charge, and that more efforts need to be made across
the EU/EEA to expand access to free ART to all migrants.
The scientific panel were asked for their opinion on the evidence relating to feasibility, acceptability, cost (resource
use), and equity of HIV screening among migrants. The results of the FACE survey showed a:
• a high level of agreement (87%) that HIV testing among migrants is a priority in the EU/EEA;
• a high level of agreement (80%) that HIV testing among migrants is feasible in the EU/EEA;
• a high level of agreement (93%) that HIV testing among migrants is acceptable in the EU/EEA; and
• a high level of agreement (93%) that HIV testing among migrants is equitable in the EU/EEA.
The ad hoc scientific panel also agreed that there are additional considerations that need to be taken into account
when offering HIV testing to migrant populations. The panel emphasised that testing be voluntary and that access
to treatment should be available as part of the testing process. Migrants may require a language interpreter and
community rapid testing programmes to improve uptake and repeat of testing. Offering testing to migrants arriving
from countries and populations with a high prevalence of HIV should be a priority.
ECDC assessment
Priority groups for testing include all adolescents and adults from high-prevalence countries (≥1%). As a significant
proportion of diagnosed cases of mother-to-child transmission of HIV and HBV are reported among migrants from
high-prevalence countries, pregnant migrant women from these countries are a priority group for screening (180).
All HIV-positive patients should immediately be linked to HIV care and treatment programmes in accordance with
WHO (180) and EACS clinical guidelines (181). In time-constrained settings, targeted rapid tests should be used to
identify HIV-positive patients. Significant data gaps limit the ability to prioritise HIV testing in communities and
primary care settings. However, despite these limitations, the benefits of HIV testing are likely to outweigh the
harms and costs if targeted to migrants originating from communities with high prevalence of HIV or at high risk of
exposure.
Evidence-based statement 1
Offer HIV screening to migrants who have lived in communities with high prevalence of HIV (≥1%). If HIV
positive, link to care and treatment as per clinical guidelines.
(Certainty of evidence: low)
Evidence-based statement 2
Offer testing for HIV to all adolescents and adult migrants at high risk for exposure to HIV. If HIV positive, link
to care and treatment as per clinical guidelines.
(Certainty of evidence: low)

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
26
Table 9. Evidence synthesis and guidance for HIV testing in migrants
Effectiveness
Cost-effectiveness
Certainty
of
evidence
(GRADE)
FACE survey*
Strength of
recommendation
Implementation
considerations
Laboratory testing of
HIV is >99%
sensitive and specific
(160). Rapid HIV
tests also report
high screening
accuracy and
community
effectiveness studies
and a systematic
review (150) have
shown higher uptake
for these tests,
notably in
communities with
moderate to high
HIV prevalence
rates.
Antiretroviral
treatments are
highly effective, and
modern combination
treatment is shown
to reduce morbidity
and mortality (162,
163)
There is very little
data on the cost-
effectiveness of HIV
testing in migrant
populations in the
EU/EEA.
Studies done in the
US, Australia and
Canada have
demonstrated that
rapid and
community testing
combined with HIV
treatments is cost-
effective in high
prevalence
populations >1%;
some studies
suggest as low as
0.1%. Programmes
may use country of
origin prevalence as
guide (see Figure 4).
Low
The ad hoc
scientific panel
rated HIV
screening among
migrants in the
EU/EEA as follows:
• High priority
• High
agreement
that screening
is feasible
• High
agreement
that screening
is acceptable
• High
agreement
that screening
is equitable.
Conditional
recommendation
based on prevalence
in country of origin
(>1%) and
prevalence in
migrants’ community
in host country.
There are gaps in HIV testing
services for migrants in the
EU/EEA, irregular
(undocumented) migrants, in
particular, face difficulties in
accessing services, and all
migrants may face barriers to
screening and treatment.
Address contributing
structural/organisational
barriers include lack of funding
for treatment, limited
availability of community-
based
services, limited entitlement to
health services.
* FACE categories were classified by the level of agreement of the panel as follows; high (>75% of ad hoc panel),
med
ium/moderate (50–75%), and low (<50%).
Evidence gaps and future research needs
There are few migrant-specific HIV screening and cost effectiveness studies in the EU/EEA. Future research should
study testing in community and primary care settings for high-risk migrant populations. As evidence is emerging of
the importance of post-migration HIV acquisition many years after arrival to the EU/EEA (106, 152, 182-184), more
research is needed to understand better the determinants of risk and which migrant populations are particularly
vulnerable to HIV acquisition. This information is critical to inform and tailor testing, prevention and policy
programmes targeted to at-risk migrant populations.
Recommendations from other national and international guidelines
Table 10. HIV screening recommendations for migrants in selected low-HIV-prevalence countries
Country
When, how and who to test
Australia (9)
Offer HIV serology to all refugees greater than or equal to 15 years of age.
Those with positive tests should be referred to a local HIV provider.
Canada (5)
• HIV serology, pre-arrival government screening programme for all immigrants and refugees of ≥ 15 years.
• Clinical screening: offer HIV serology to high-risk migrants, with informed consent.
• All adolescents and adults from countries where HIV prevalence is ≥1% (sub-Saharan Africa, parts of the
Caribbean and Thailand).
• Link HIV-positive individuals to HIV treatment programmes and post-test counselling.
France (185)
• Yearly HIV screening is recommended for migrants originating from countries of high prevalence, especially
sub-Saharan Africa and the Caribbean.
• HIV screening recommended in association with HBV and HCV screening for migrant populations.

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
27
Country
When, how and who to test
Ireland (8)
Offer test for HIV Ag/Ab to the following groups:
• All women attending antenatal services.
• All those with risk factors for HIV, including but not limited to:
- people from high-HIV-prevalence countries (>1%)
- people with concurrent sexually transmitted infections
- people who inject drugs
- sex workers and those who have been trafficked
- men who have sex with men (MSM)
- people with concurrent TB infection
Refer all positive cases to specialist services for review.
Italy (13)
During the second phase of reception, offer all migrants culturally sensitive counselling for HIV.
Offer HIV tests to:
• all migrants aged ≥ 16 years coming from high-prevalence (1%) countries
• pregnant and breast-feeding migrant women
• those exposed to high risk (blood transfusions in country of origin, sexually abused people, or people with
multiple sexual partners
• people with concomitant presence of active TB or IST.
Migrants < 16 years should be offered an HIV test if they meet at least one of the below criteria:
• born from HIV-positive mothers
• early sexual activities
• history of sexual abuse
• concomitant presence of active TB or IST.
UK (186, 187)
HIV testing in the UK is recommended in selected specialist services, in certain clinical, community and home
settings where there is risk of transmission to others, and for high risk groups.
High-risk groups include people born in a country of high diagnosed HIV prevalence (>1%), those reporting
sexual contact with people from countries of high HIV prevalence and black African populations.
For all high risk groups, routine testing is recommended annually if negative.
US (10)
• Post arrival (not mandatory prior to arrival)
• HIV test, universal
• Testing of all refugees is encouraged. Annual testing should be offered to all (including immigrants/migrants).
Repeat testing annually for those from high-prevalence regions and those engaging in high-risk behaviours.
• Refer to specialist, post-test counselling.

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
28
4.4 Hepatitis B
Burden of disease
Hepatitis B virus (HBV) is a public health priority for the (EU/EEA). HBV is a vaccine-preventable and treatable
communicable disease. In 2013, five European countries reported a high population prevalence (≥2%) (188) of
chronic hepatitis B infection (CHB): Bulgaria (4.25%), Greece (2.33%), Romania (5.49%) (189), Lithuania
(2.03%), and Slovenia (3.29%) (190).
CHB is highly prevalent in several areas of the world, notably Africa and Asia (Figure 3). Of the 49 million foreign-
born people living in the EU/EEA, it is estimated that approximately 53% come from a country of intermediate/high
endemicity (190). The average prevalence of CHB in migrants living in the EU/EEA that were born in an HBV-
prevalent country is 5.5%, compared with an overall prevalence of 1.12% in the general EU/EEA population (27).
The prevalence of CHB is higher in migrants who were refugees or asylum seekers compared with all migrants
(9.6% vs. 5.1%) (191). Antenatal screening programmes in Europe report that migrant women account for 1.0 to
15.4% of all antenatal diagnoses of CHB, with an average prevalence that is six times higher than the indigenous
female EU/EEA population (192). ECDC estimates that migrants from countries where HBV is highly prevalent
(≥2%) account for 25% of all HBV infections in the EU (27) (Figure 3).
Vaccination and screening practices vary across the EU/EEA. Seven of 21 EU/EEA countries for which information
was available have a national policy for screening migrants for HBV (193). By contrast, universal HBV screening in
antenatal screening programmes is national policy in 23 of 26 countries (194). In 27 of the 31 EU/EEA countries,
universal childhood HBV vaccination is recommended, and all 31 countries recommend vaccination for children in
high-risk groups.
Figure 3. Estimations of worldwide prevalence of chronic hepatitis B virus infection
Source: Estimations of worldwide prevalence of chronic hepatitis B virus infection: a systematic review of data published between
1965 and 2013 (195)
Summary of evidence
Effectiveness
As stated in the methods section (Section 3.4), studies on high-risk migrant groups were prioritised. When migrant-
specific studies were lacking, indirect evidence (i.e. studies on general populations which can be extrapolated to
interventions that are targeted toward migrants) was used. Where evidence from non-migrant populations was
used, input from the expert panel regarding the applicability and validity for migrant populations was sought, and
the indirectness of the evidence was reflected in the evidence grade.
Using the analytic framework for the systematic review (22), four systematic reviews (191, 196-198) and five
additional studies and guidelines were identified (190, 199-202) that reported on the effectiveness of HBV
screening, vaccination and treatment programmes
. No RCTs on the effectiveness of screening migrants for HBV
were found. Two systematic reviews (196, 197) and two clinical guidelines (200, 201) were identified that report on
evidence relevant to the effectiveness of CHB treatment.

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
29
Serological tests for HBV screening are considered highly accurate (sensitivity and specificity of >98% for detecting
hepatitis B surface antigen) (190). Treatment for chronic infection with interferon-alpha versus no
treatment/placebo decreased hepatic events, defined as hepatocellular carcinoma (HCC), and liver-related mortality
(RR 0.55 (95% CI 0.43–0.70); p<0.001)) and cirrhotic complications, defined as ascites, hepatic encephalopathy,
variceal bleeding and hepatorenal syndrome (RR 0.46, 95% CI 0.32–0.67, P<0.001) (197). Treatment with
nucleotide analogues resulted in improvement in intermediate markers of chronic HBV infection including loss of
HBsAg compared with placebo RR 2.39 (95% CI 1.16 to 4.94) (196). The 2017 Clinical Practice Guidelines by the
European Association for the Study of Liver Disease (EASL) recommends the use of the nucleotide analogues as
first-line therapy for chronic HBV (200).
An effective vaccine for hepatitis B has been available for several decades and has been shown to have reduced
the prevalence of HBV globally (201, 203-205).
Cost-effectiveness
We included nine studies on cost-effectiveness of screening and vaccination (206-214). A Dutch modelling study
among a cohort of people with HBV infection comparing the natural history of infection with one-off screening for
HBsAg and treating active cases of CHB with entecavir, resulted in an incremental cost-effectiveness ratio (ICER) of
screening and treatment compared with no formal screening, of EUR 8 966 per quality-adjusted life year (QALY)
gained, with a range of EUR 7 222 to EUR 15 694 in a sensitivity analysis. These values are well below the
commonly-used Dutch cost-effectiveness threshold of EUR 20 000 per QALY gained (209).
Among the five studies of migrants to North America, the costs ranged from CAD 6 077 (192) to USD 86 620 (208)
per person screened (and treated in the event of a positive result), with the majority of studies estimating
programme costs of >USD 20 000 per person per year. Thus, the costs of these interventions were generally
considered moderate. The ICER of screening and treatment for HBV, compared to no screening, ranged from USD
36 088 (208) to CAD 40 880 (192) and CAD 101 513 (EUR 72 508] (207) per quality-adjusted life year (QALY)
gained. Screening was generally considered cost-effective at the host countries’ commonly accepted willingness-to-
pay thresholds. Therefore, all cost-effectiveness studies favoured screening and treatment for HBV over the status
quo of no (or voluntary) screening. A study found that HBV screening was likely to be cost-effective for populations
with a prevalence of HBV ≥2% (207). Two studies of outpatients to US hospitals found that screening may be cost-
effective even in populations with a lower than 2% prevalence (0.3%) (215).
Three studies from North America reported on the cost-effectiveness of HBV vaccination compared with no
vaccination in adults in mixed populations, including >50% migrants from south Asia and sub-Saharan Africa.
These studies found that screening and vaccination in adults was not cost-effective or dominated by the screen and
treat strategies (192, 207, 208). Vaccination provides little incremental health benefit for the additional vaccination
costs, because vaccination does not change the health outcomes of persons with an existing chronic infection, and
prevents only few chronic infections, as an acute HBV infection in adulthood leads to chronic hepatitis in less than
5% of cases (208).
Implementation considerations
Migrants, including refugees, have been shown to accept the value of hepatitis B vaccination (93). Qualitative
studies also suggest some migrants will seek HBV screening to gain reassurance or to prevent liver disease (216,
217), but that in some groups there is considerable lack of awareness of this infection (218). Fear of discrimination,
stigma, loss of income or social status may, however, decrease uptake of screening and willingness to return for
results and/or follow-up appointments (217); screening programmes for HBV will need to consider targeting a
wider group of migrants circulating in the EU/EEA, a substantial number of whom will have come from intermediate
and/or high endemic areas for HBV. HBV screening programmes have begun to consider community screening
approaches and linkage to monitoring and treatment. Qualitative studies report multiple community-based testing
strategies (219) for HBV; for example, mobile and home testing (220), internet-based testing (221), and testing in
workplaces (222), street festivals (223), restaurants and bars (223), places of worship (224) and educational
establishments (225). Recent focus has been placed on multi-disease testing in the primary care context, targeting
migrants and offering one blood test for multiple infections in one appointment (HBV, HCV, HIV, latent TB) (215).
A recent systematic review found uptake by migrants to be high to HBV screening initiatives in the EU/EEA (median
uptake 87.39% (range 32.34–100.00%)), suggesting acceptability towards HBV screening (93) (supported by other
studies (226)). Screening uptake was highest in programmes that involved community partners or received the
endorsement of local groups (219). A study of Chinese migrants in the Netherlands offered screening in schools,
community centres and churches or at the local public health clinic, with support from migrants for community-
based screening and outreach programmes (225).

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
30
Ad hoc scientific panel opinion
The scientific panel was in agreement that HBV screening should be prioritised for migrants coming from high-
prevalence countries, as it allows for early detection and treatment, reduces individual morbidity, and prevents
onward HBV transmission. The strength of the recommendation was deemed conditional on the estimated
prevalence of chronic HBV in migrants’ country of origin, except in the case of pregnant women, where testing is
recommended for all pregnant women irrespective of the prevalence in the country of origin. The panel endorsed
vaccination of migrant children and adolescents as an effective public health option to prevent HBV infection and
the chronic sequelae of infection. This applied to both migrant children from HBV-endemic countries and other
countries as per EU/EEA country childhood vaccination schedules.
The scientific panel were asked for their opinion on the evidence relating to: feasibility, acceptability, cost (resource
use), and equity of hepatitis B screening among migrants. The results of the FACE survey showed the following:
• High level of agreement (87%) that hepatitis B screening and vaccination among migrants is a priority in
the EU/EEA.
• Medium level of agreement (63%) that hepatitis B screening and vaccination among migrants is feasible in
the EU/EEA.
• High level of agreement (76%) that hepatitis B screening and vaccination among migrants is acceptable in
the EU/EEA.
• High level of agreement (79%) that hepatitis B screening and vaccination among migrants is equitable in
the EU/EEA.
The ad hoc scientific panel agreed that the evidence was of very low to low certainty, but chronic HBV is a
potentially treatable disease and the panel felt that early detection may improve outcomes. The panel agreed that
vaccination is a priority and that, ideally, catch-up vaccination programmes should be implemented. Programmes
should also focus on linking migrants with chronic HBV to monitoring and treatment, overcoming barriers to care
such as loss of income, loss of status, and stigma.
ECDC assessment
Chronic hepatitis B is a communicable public health priority in the EU/EEA. The disease can be prevented and
treated to prevent liver cancer and cirrhosis. The WHO goal of elimination of viral hepatitis as a public health
concern by 2030, which the EU has committed to achieve, requires a significant increase in the proportion of
people living with CHB who are diagnosed, linked to care, and offered antiviral treatment. Available serological
tests are sensitive and specific, and current therapies are effective at reducing progression to cirrhosis and liver
cancer. Therefore, countries should consider screening migrants from countries with a HBsAg prevalence >2% for
hepatitis B infection and immunity. Those who remain susceptible should be offered vaccination (in accordance
with national guidelines), with priority for children and adolescents, and adults with additional risk factors
(including people who inject drugs, MSM, people with multiple sexual partners). Testing should be offered to all
household contacts and sexual partners of those diagnosed with CHB. Testing is recommended for all pregnant
women irrespective of the prevalence in the country of origin.
Evidence-based statement 1
Offer screening and treatment for hepatitis B (HBsAg and anti-HBc, anti-HBs) to migrants from intermediate-/high-
prevalence countries (≥2% to– ≥5% HBsAg).
(Certainty of evidence: low)
Evidence-based statement 2
Offer hepatitis B vaccination series to all migrant children and adolescents from intermediate-/high-prevalence
countries (≥2% to– ≥5% HBsAg) who do not have evidence of vaccination or immunity.
(Certainty of evidence: low)

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
31
Table 11. Evidence synthesis and guidance for hepatitis B vaccination and screening in migrants
Effectiveness Cost-effectiveness Certainty
of
evidence
(GRADE)
FACE survey* Strength of
recommendation
Implementation
considerations
No RCT level evidence was
found on screening
programs for HBV. No
direct evidence was found
for the effectiveness of
HBV vaccine or screening
programmes in migrants.
Serological markers are
˃98% sensitive and
specific for detecting
hepatitis B surface antigen
(190).
Evidence of antiviral
effectiveness at reducing
progression to cirrhosis
and liver cancer noted.
Studies report a reduction
in prevalence of HBV
following vaccination in
infants, children, health
workers, and indigenous
populations (198, 227-
229). The degree of
effectiveness varied
between studies.
Screening is likely to be
cost-effective, even in
low-prevalence
populations (>0.3%)
(207, 215).
Vaccination of adults
without additional risk
factors may provide
little incremental health
benefit for the
additional costs (208).
Universal vaccination,
compared to no
vaccination among low-
risk adult populations,
does not appear to be
cost-effective (192,
208, 211).
low
The ad hoc scientific
panel rated HBV
screening, treatment
and vaccination
among migrants in
the EU/EEA as
follows:
• High priority
• Moderate
agreement that
screening is
acceptable
• High agreement
that screening is
feasible
• High agreement
that screening is
equitable
Conditional
recommendation for
screening migrants
from intermediate and
high-prevalence
countries.
Strong
recommendation for
vaccination of migra
nt
children and
adolescents.
Migrant barriers in
accessing healthcare
contribute to
decrease
screening uptake and
willingness to disclose
hepatitis test results
(217).
Screening uptake is
highest in
programmes that
involve community
partners or the
endorsement of local
groups (219).
Programmes
screening for CHB
should consider
linkage of cases to
monitoring and
treatment.
Migrant women
should be screened in
existing antenatal
programmes.
* FACE survey high level of agreement (>75% of scientific panel), medium level of agreement (50–75% of scientific panel), and
low level of agreement (<50% of scientific panel).
Evidence gaps and future research needs
Community-based screening studies and related cost-effectiveness studies on migrant populations are required to
determine the optimal approach to improve uptake and linkage to monitoring and care. Studies on acceptability
and feasibility in the EU/EEA on various high-risk migrant groups are needed to build trust and knowledge to
support the testing approach. Research is needed to improve strategies to ensure that vaccination programmes
reach all migrant children and adolescents.

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
32
Recommendations from other national and international guidelines
Table 12. HBV screening recommendations for migrants in selected counties
Country
Who when, how to test/assess
Australia (9)
• Screening for hepatitis B infection should be offered to all refugees and for all people born in countries
with a HBsAg prevalence >2%.
• For those diagnosed with chronic hepatitis B: linkage to care, including additional tests, monitoring and
treatment. Test household and sexual contacts, vaccinate those susceptible.
Canada (5)
• Screen adults and children from countries where the seroprevalence of chronic hepatitis B virus
infection is moderate or high (i.e. ≥ 2% positive for hepatitis B surface antigen), such as Africa, Asia
and eastern Europe, for hepatitis B surface antigen, anti-hepatitis B core antibody and anti-hepatitis B
surface antibody.
• Refer to a specialist if positive for hepatitis B surface antigen (chronic infection).
• Vaccinate those who are susceptible (negative for all three markers).
France (230)
• Screening for hepatitis B is recommended for migrants in association with HCV and HIV testing.
Vaccinate against hepatitis B in accordance with existing French recommendations.
Ireland (8)
• Offer testing to all new migrants originating from countries with a HBsAg prevalence of ≥2%; all
women attending antenatal services; household or sexual contacts of cases; people who engage in
high risk behaviours.
• Refer positive cases to specialist services; vaccinate all children <10 years of age; vaccinate all
migrants from countries with a HBsAg prevalence ≥2%; vaccinate non-immune, high-risk persons.
Italy (13)
During the second phase of the reception, offer screening (HBsAg, HBsAb, HBcAb) to all migrants from
countries with HBsAg prevalence >2%.
• Regardless of the country of origin, offer tests to migrants who meet at least one of the below criteria:
- concomitant HIV infection
- previous blood transfusion
- intravenous drug addiction
- multiple sexual partners
- victim of sexual abuse
- close contact with HBsAg-positive relatives
- under immunosuppressive treatment
- pregnancy
Screening should cover HBsAg, HBcAb e HBsAb.
In the case of seropositivity to HBsAg, the patient should be sent to a specialist for follow-up and
treatment.
UK (231-233)
Pre-departure for refugees entering through resettlement programmes, and post-arrival for other migrants
(including asylum seekers):
• Hepatitis B testing should be offered to people who were born, brought up in, or resided for a
substantial amount of time in countries with an intermediate or high prevalence of chronic hepatitis B
infection (2% or greater).
• Testing should also be offered to sexual and family contacts of persons known to be infected with
hepatitis B and to people with other risk factors (such as high number of sexual exposures, illicit drug
use, among others).
• Vaccination for newly arrived migrant infants with uncertain vaccination status is recommended up to
first birthday.
USA (142)
• Tested/vaccinated prior to and/or following arrival. Refugees or immigrants who are from, or have lived
in, countries with prevalence of chronic HBV infection ≥2% or those in high-risk groups should be
tested for infection (HBsAg). If negative, vaccination should be offered or serologies should be
checked, with vaccination offered to those who are non-immune.
• Counselling and evaluation for treatment. Vaccinate household contacts.

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
33
4.5 Hepatitis C
Burden of disease
Chronic hepatitis C (CHC) is an important public health problem in the EU/EEA and a leading cause of chronic liver
disease and preventable economic burden (234-236). As the infection is largely asymptomatic, people affected
often remain undiagnosed and untreated, which may result in progression to cirrhosis and liver cancer (237). The
recent advent of short course, orally administered and well-tolerated direct-acting antiviral (DAA) therapies that
cures hepatitis C virus (HCV) infection in >95% of cases provides a historic opportunity to address the burden
associated with this disease (238). An estimated 3.9 million people in the EU/EEA have CHC infection, with HCV
prevalence in EU/EEA countries ranging from 0.1–5.9% (239, 240). Despite the high burden of CHC in the EU/EEA,
a modelling study estimated that only 36.4% of people living with CHC have been diagnosed; of these, 12.7%
have been treated (239). Europe has endorsed and is committed to the WHO goal to eliminate hepatitis C as a
public health threat by 2030 (241). The European hepatitis action plan aims to achieve high uptake along all steps
of the HCV ‘care cascade’ (diagnosis, linkage to care, treatment and cure) for all populations at risk (241).
HCV screening and control programmes in the EU/EEA primarily focus on groups with traditionally recognised risk
factors such as people who inject drugs, as they experience the greatest burden of disease (239). Migrants from
HCV-endemic countries (anti-HCV prevalence of ≥2%) are an additional group in the EU/EEA at increased risk of
CHC. Migrants from these countries have an average anti-HCV prevalence of 2% and account for a
disproportionate number of all HCV cases (14%) in the EU/EAA and up to a half of those living with CHC in some
low-HCV-prevalence EU/EEA countries (27). In 2016, the EU/EEA received approximately two million migrants from
outside of the EU/EEA, almost 80% of whom are believed to have originated from HCV-endemic countries, with an
HCV prevalence generally similar to that in their countries of origin (Figure 4) (27, 242-246).
Figure 4. Prevalence of anti-HCV globally in 2015
Source: (247)
Summary of evidence
Migrants bear a disproportionate burden of HCV in many EU/EEA countries. They are more likely to have been
exposed to HCV in their countries of origin through unsafe injections, unsafe medical procedures, or unscreened
blood products; however, they are less likely than the native-born #198; #261; #262}. Migrants are older and
more likely to have advanced liver disease and hepatocellular carcinoma compared with non-migrants at the time
of HCV diagnosis (248-250). This is likely to be due to missed or delayed diagnoses and possibly infection at an
earlier age than is the case for other people living with CHC.
In a study from Finland, 62.5% of migrants found to be HCV positive had not been previously diagnosed. In a
population-based Canadian study, it took a mean of 10 years after arrival for migrants to be diagnosed with HCV
(249, 251). These data suggest that early screening based on HCV prevalence in the country of origin together
with linkage to care and treatment could prevent liver-related sequelae in the migrant population. However, few
EU/EEA countries have national guidance on testing migrants for HCV (193).

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
34
Effectiveness
As stated in the methods section (Section 3.4), studies on high-risk migrant groups were prioritised. However,
when migrant-specific studies were lacking, indirect evidence (i.e. studies on general populations which can be
extrapolated to interventions that are targeted toward migrants) was used. Where evidence from non-migrant
populations was used, input from the expert panel regarding the applicability and validity for migrant populations
was sought, and the indirectness of the evidence was reflected in the evidence grade.
The data identified in this review support the effectiveness and cost-effectiveness of HCV screening in populations
at risk for HCV infection, including for migrants originating from intermediate and high-HCV-prevalence countries
(anti-HCV ≥2% and ≥5%, respectively] (23)
. We included five systematic reviews and one set of guidelines that
addressed the HCV screening chain of evidence; two assessed the performance of HCV diagnostic tests (190, 252),
three assessed the impact of HCV treatment on preventing HCC and all-cause mortality (n = 3) (253-255) and one
considered uptake along all steps of the HCV care continuum (256).
The performance of diagnostic testing for HCV has been summarised in the 2017 WHO Guidelines on Hepatitis B
and C testing (190). In populations from low-, middle- and high-income countries WHO estimates the sensitivity
and specificity of third-generation HCV EIAs to be 98% and 99%, respectively (190). Point-of-care tests, a strategy
that potentially could increase screening uptake, was found to perform well in populations from low-, middle- and
high-income countries (252).
The new DAA regimens are the recommended therapy for all HCV genotypes in the EU/EEA. These regimens are
well tolerated and cure >95% of infections, defined as achieving sustained viral response (SVR) or negative HCV
RNA, 12 weeks after completing treatment, which is considered to be a reliable surrogate outcome (200, 238).
Despite highly sensitive and specific tests to detect HCV and curative HCV therapies, the HCV care cascade in the
pre-DAA era was weak (256). In a systematic review of studies of the HCV care continuum in the US from 2003–
2013, for example, only 50% of cases were diagnosed and aware of their infection, 27% had HCV RNA
confirmatory testing, 16% were prescribed HCV therapy, and 9% achieved SVR (256). A modelling study in Europe
published after the search timeframe also demonstrated a weak HCV care continuum: in 2015, only 36.4% of all
HCV cases in the EU/EEA were diagnosed, and of these, only 12.7% were treated (237).
Cost-effectiveness
Simplified, shorter duration (8–12 week) pangenotypic DAA regimens are now widely recommended for most HCV
infections (200). We included six studies that assessed the cost-effectiveness of HCV screening followed by DAA
therapy and eight studies that assessed the cost-effectiveness of DAA therapy, all conducted before our search end
date in 2016.
Screening for HCV in those treated with DAAs is cost-effective, even at higher 2015 costs. A UK study found that
screening pregnant women attending antenatal clinics and treating them following delivery was cost-effective
(257). The incremental cost-effectiveness ratio (ICER) for screening and treatment compared with no screening
and no treatment was GBP 2 400 (EUR 2 745) per QALY gained. For screening and treating with DAAs compared
with no screening and no treatment, the ICER was still cost-effective at GBP 9 139 (EUR 10 455) per QALY gained.
A Canadian study also found that screening for HCV in different age groups and then treating with DAAs was cost-
effective (207). The ICER for IFN-free DAAs vs. older therapies ranged from CAD 34 359 (EUR 21 977) to CAD
44 034 (EUR 28 166) per QALY gained. The same group published a paper after our search timeframe and found it
was cost-effective to screen immigrants from HCV-endemic countries (defined as a seroprevalence of 1.9%) with
an ICER of CAD 31 468–34 600 (EUR 20 375–22 403) per QALY gained (258).
Non-pangenotypic DAA therapies were found to be moderately cost-effectiveness in France but had a large budget
impact at the 2015 cost of treatment (259). Deuffic-Burban found that DAAs were moderately cost-effective for
genotype 1 and 4 at a median threshold of EUR 24 000 per QALY gained and a maximum upper limit of EUR
80 000 per QALY gained; however, wide-scale introduction of these regimens would cost EUR 3.5–7.2 billion. IFN-
based regimens were estimated to be more cost-effective for genotypes 2 or 3 at EUR 21 300 to EUR 19 400 per
QALY gained regardless of fibrosis stage. Several US studies have also evaluated the cost-effectiveness of DAA
therapies compared with older PEG-INF-RBV therapies and found that DAA therapies were moderately cost-
effective at a willingness-to-pay threshold of USD 50 000 US (EUR 39 210), but varied significantly by HCV
genotype, presence of liver fibrosis, and treatment history (260-265). As the cost of DAA therapies has declined in
the EU/EEA over the past two years, CHC treatment is now more affordable, more widely available, and more cost-
effective (266-268). With the decrease in DAA costs and the availability of highly effective pan-genotypic
medications, HCV screening and DAA therapy is likely to be more cost-effective among persons with all HCV
genotypes than the estimates from the studies described above.

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
35
Implementation considerations
The tools to achieve HCV elimination in the EU/EEA are available although there are a number of implementation
challenges, including identifying all persons at HCV risk and linking those affected to care and treatment. Migrants are
disproportionately affected by HCV in some EU/EEA countries and face multiple barriers to accessing healthcare
services. Barriers include lack of knowledge and awareness of risk, fear and stigma associated with blood-borne
diseases, and socio-economic, linguistic and cultural barriers (177, 269, 270). Screening uptake for HCV has been
found to be high in migrant populations in the EU/EEA (median 78.59% (range 32.34-96.77)) (93). HCV screening
uptake and linkage to care can be improved by implementing decentralised community-based screening strategies
and working with community-based organisations to overcome cultural and language barriers (271-275), or using
multi-disease testing approaches whereby HCV testing is offered as a blood test alongside HBV, HIV, and latent TB
(215). High rates of screening uptake and of treatment initiation and completion were observed in programmes using
community-based screening strategies (272, 274). The EU-HEP SCREEN pilot project implemented community
outreach and opportunistic screening in primary care to target migrants in England, Hungary, Scotland and Spain, with
rates of screening uptake ranging from 33% to 80% and the highest uptake in primary care opportunistic screening
(271, 276). Similarly, the CDC HEP-TLC programme and the Hepatitis Outreach Network (HONE) programme in the
USA engaged community-based organisations, and employed outreach workers in non-traditional venues to reach
migrant communities. These programmes achieved high levels of screening (50–60%) and linkage to care (65%)
(274, 277). Furthermore, an RCT compared integrated point-of-care testing for HCV, HBV, and HIV in primary care
among migrants with individual serological testing and found that testing uptake (98% vs. 62%) and linkage to care
(90% vs. 83%) was higher among point-of-care testing (278).
The WHO recommends screening persons originating from countries with an intermediate (≥2%) and high (≥5%)
HCV prevalence (190). Recent guidance from the WHO Regional Office for Europe has highlighted the need to
increase diagnosis of people living with CHC and linkage to care while taking into consideration the local epidemiology
of CHC in groups at risk, the capacity of existing systems, and leveraging already existing prevention and control
efforts (204). Each country should assess its capacity to increase HCV testing in at-risk populations, link those living
with CHC to care and provide access to HCV treatments. HCV screening and treatment programmes for migrants in
the EU/EEA will need to be tailored to their specific needs as well as ensuring universal access to healthcare so as to
enhance effectiveness along the entire HCV care continuum.
Ad hoc scientific panel opinion
The scientific panel members agreed that screening migrant populations for HCV is an important strategy that
should be considered in the EU/EEA. Feasibility, cost of new treatment options and limited evidence on migrant
screening programmes were identified as concerns. The panel concluded that the strength of the recommendation
for HCV screening among migrants and linking and treating those found to be positive was conditional on the
prevalence of hepatitis C in the migrants’ country of origin.
The scientific panel were asked for their opinion on the evidence relating to: feasibility, acceptability, cost (resource
use), and equity of HCV screening among migrants. The results of the FACE survey showed a:
• Medium level of agreement (75%) that HCV testing among migrants is a priority in the EU/EEA.
• Low level of agreement (40%) that HCV testing among migrants is feasible in the EU/EEA.
• Medium level of agreement (60%) that HCV testing among migrants is acceptable in the EU/EEA.
• Medium level of agreement (67%) that HCV testing among migrants is equitable in the EU/EEA.
Although the ad hoc scientific panel agreed that hepatitis C was a priority for the EU/EEA, screening and treating
migrants requires addressing cultural and language issues and may, therefore, increase the complexity of
programmes. The acceptability of screening and treatment is highly dependent on the cultural sensitivity of and
sense of trust in healthcare professionals and their recommendations.
ECDC assessment
Chronic hepatitis C is an important public health problem in the EU/EEA. The disease leads to cirrhosis and liver
cancer in a substantial proportion of people living with undetected and untreated CHC. To address the growing
burden of HCV in the EU/EEA and achieve the WHO goal of elimination of viral hepatitis as a public health concern
by 2030, those affected should be diagnosed and linked to care and treatment. Migrants originating from HCV-
Evidence-based statement
Offer hepatitis C screening to detect HCV antibodies to migrant populations from HCV-endemic countries (≥2%)
and subsequent RNA testing to those found to have antibodies. Those found to be HCV RNA positive should be
linked to care and treatment.
(Certainty of evidence: moderate)

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
36
endemic countries have a higher prevalence for HCV than the native-born population and account for up to a half
of the cases in low-HCV-prevalence EU/EEA countries. Highly sensitive and specific tests to detect HCV and curative
HCV therapies, although expensive, are available but impact is limited by weaknesses in the HCV care continuum
(diagnosis, linkage to care and treatment completion). Lower costs of DAA have made these treatments more
available and cost-effective. Patient and provider barriers that contribute to low uptake and losses across the HCV
care cascade need to be addressed. The effectiveness of HCV screening may be increased through integration with
screening for other diseases, such as HIV and HBV, and through the use of community-based and culturally and
linguistically adapted approaches to service delivery.
Table 13. Evidence synthesis and guidance for hepatitis C screening in migrants
Effectiveness Cost-
effectiveness
Certainty
of
evidence
(GRADE)
FACE survey* Strength
recommendation
Implementation
considerations
Enzyme immunoassays
(EIAs) are highly
sensitive (98%) and
specific (99%) to
detect anti-HCV
antibodies (190).
EIA point-of-care
testing is almost as
sensitive and specific as
blood-based testing
and may be more
convenient for the
patient (252).
Both tests need to be
confirmed with a
nucleic acid test (NAT)
to ensure the presence
of active virus (190).
DAA therapy is curative
in most patients
(>95%) and is well
tolerated but is very
expensive (238).
Despite excellent
diagnostic tests and
therapies,
the HCV care
cascade in the pre-
DAA
era was weak, with
only ~35% of patients
being diagnosed and
16% offered therapy
(256).
In France, DAAs
were moderately
cost-effective for
genotypes 1 & 4,
ranging from EUR
40 000 to EUR
88 000 per QALY
gained, whereas
IFN-RBV was more
cost-effective for
genotypes 2 & 3.
Introducing DAA
regimens on a wide
scale would have a
substantial budget
impact of EUR 3.5-
7.2 billion at the
2015 cost of therapy
With lower DAA
costs, HCV
screening and DAA
therapy is more
cost-effective than
the estimates from
the included studies.
Moderate
HCV screening
among migrants in
the EU/EEA was
rated as follows:
•
Medium
priority
•
Low
agreement
that screening
is feasible
•
Moderate
agreement
that screening
is acceptable
•
Moderate
agreement
that screening
is equitable.
Conditional
recommendation
based on
intermediate to high
HCV prevalence
(≥2%) in country of
origin.
Migrants bear a
disproportionate burden of
HCV in the EU/EEA; patient,
provider and health system
barriers need to be
addressed to ensure high
uptake along the entire HCV
care continuum.
At the patient level,
addressing stigma and
cultural and linguistic barriers
will be required.
Providers will need to be
educated about the
importance of screening
migrants from intermediate-
and high-HCV-endemic
countries for HCV.
* FACE categories were classified by the level of agreement of the panel in the following manner; high (>75% of ad hoc panel),
med
ium (50–75%), and low (<50%).
Evidence gaps and future research needs
Although DAA regimens are now recommended for all HCV genotypes in the EU/EEA (200), there is no specific
data on the effectiveness or cost-effectiveness of screening and treating with these medications in migrants in the
EU/EEA. There are also few studies on uptake across the HCV care continuum in different EU/EEA countries in the
DAA era. Finally, there is little data on the liver-related outcomes, deaths and economic burden due to
undetected/untreated HCV among migrants in the EU/EEA.

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
37
Recommendations from other national and international guidelines
Table 14. Hepatitis C screening recommendations for migrants in selected low-HCV-prevalence
countries
Country
When, how and who to test
Australia (9) Offer testing when risk factors are present or from a country with high prevalence (>3%).
Test with anti-HCV antibodies; if positive, request HCV RNA test and link those positive to care.
Canada (5)
Recommendation is to screen with Anti-HCV antibodies for all immigrants from countries of high prevalence
(>3%); if positive, link to care
Ireland (279)
• Offer test for anti-HCV to:
− all migrants who originate from countries with a prevalence of chronic hepatitis C of ≥ 2%;
− those with a history of hepatitis C risk exposure/behaviour including people who inject drugs and
men who have sex with men.
• Offer test for HCV RNA to all those who have a positive anti-HCV result.
• Refer all positive cases to specialist services for review.
• Vaccinate those who are non-immune to hepatitis A and/or hepatitis B with hepatitis A and/or hepatitis
B vaccine.
Italy (13) During the second reception phase, offer screening tests (HCV-Ab) to all migrants coming from high HCV-
RNA-prevalence (> 3%) countries
• Regardless the country of origin, offer tests to those migrants with:
− concomitant HIV infection
− previous blood transfusion
− intravenous drug addiction
− abnormal liver tests
− risk factors for parenteral transmission
• Migrants with positive HCV-Ab test should be tested for HCV-RNA and sent to a specialised centre for
follow-up of the diagnosis and, if positive, treatment.
UK (232, 280) Offer testing by Anti-HCV antibodies to people from countries where hepatitis C is endemic (prevalence 2%
or greater) and confirm positive results with HCV RNA, either pre-entry or post-arrival.
US (142)
Offered to those with risk factors, no special targeting for immigrants from high-prevalence countries.
France (281, 282) Screening is recommended for persons originating in, or receiving care, in countries known or presumed to
have high prevalence of HCV (south-east Asia, Middle East, Africa, South America).
Expert recommendations: screening for hepatitis C is recommended for migrants in association with
hepatitis B and HIV testing.

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
38
4.6 Strongyloidiasis and schistosomiasis
Burden of disease
The public health impact of two neglected parasitic diseases, schistosomiasis and strongyloidiasis, has increased in
non-endemic regions due to increased global migration flows (283-285). Although the real burden of the disease
has always been underestimated due to poorly sensitive diagnostic methods used in low-resource settings (285),
recent estimates report that Strongyloides stercoralis infects around 370 million people globally (285). Likewise,
Schistosomiasis spp. infects more than 200 million people, causing more than 1.53 million disability-adjusted life
years (DALYs) (286-288).
Human schistosomiasis is caused by different species of the trematode Schistosoma spp., S. mansoni being the
most prevalent and distributed in Africa, America, the Middle East and the West Indies, followed by
S. haematobium in Africa and the Middle East and S. japonicum in east and south-east Asia (289). Strongyloidiasis
is caused by the nematode Strongyloides stercoralis and, although it generally occurs in subtropical and tropical
countries, it can be present in temperate countries with favourable conditions (290).
Of all helminthic infections, both schistosomiasis and strongyloidiasis have characteristics which make them
appropriate for screening. First, most infected subjects are asymptomatic (291s) and unaware of infection (292), or
complain of very mild unspecific symptoms (289). Second, both diseases are considered chronic conditions (292).
S. stercoralis replicate indefinitely inside the human host through an auto-infective cycle, causing lifelong infection
if left untreated (292). Schistosomiasis can remain as a subclinical infection for years, leading to long-term
complications (293). Third, both infections can cause potentially severe conditions. S. stercoralis can cause
disseminated infections or hyper-infections with fatal outcomes in immunosuppressed patients (293). Chronic
schistosomiasis is the result of an immune-mediated granulomatous response to trapped eggs that produces
organ-specific manifestations, which are mainly chronic urogenital and/or hepato-intestinal complications (289,
294, 295). There are little data on the burden of these diseases among migrants in the EU/EEA. Our estimates
were derived from small observational studies from selected countries.
Few studies have assessed the prevalence rate of schistosomiasis in European countries, although a recent study
shows prevalence higher than 17% in sub-Saharan African migrants (296). Prevalence of schistosomiasis in
endemic countries remains high, particularly in sub-Saharan African countries, which account for around 90% of all
reported cases annually (289). Prevalence rates of 10%–>50% for S. haematobium infections have been reported
in some sub-Saharan African countries and the Middle East (287). Prevalence rates of 1%–>40% have been
reported for S. mansoni in sub-Saharan Africa, Brazil, Suriname and Venezuela, and for S. japonicum in Indonesia,
parts of China and south-east Asia (287-289, 296, 297) (Figure 5).
For strongyloidiasis, data derived from refugee populations originating from south-east Asia and Africa showed
prevalence rates of between 0.8% and 4.3% using stool microscopy; higher rates of between 9% and 77% were
reported using serum antibody-detection assays in refugees from south-east Asia (297). In the EU/EEA, prevalence
rates of strongyloidiasis of 3.3%, 4.2% and 5.6% were reported in Italy, Spain and France, respectively, mainly in
migrant populations or expatriates, without any reference to the diagnostic methods (297).
There are no standard EU guidelines or recommendations for the screening and treatment of schistosomiasis and
strongyloidiasis and few examples of practice. Ireland and the UK are the only EU/EEA countries with a published
infectious disease assessment for migrants or refugees (in the case of the UK) that includes general guidance for
screening and treatment of schistosomiasis and strongyloidiasis and other intestinal parasites in asymptomatic
people (8, 232, 298). Other countries with published policies include the US, Canada and Australia (5, 299, 300).

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
39
Figure 5. Distribution of schistosomiasis, worldwide (2012)
Source: WHO. Available from:
= http://www.who.int/schistosomiasis/Schistosomiasis_2012-01.png
Summary of evidence
Effectiveness
We developed an analytical evidence framework for screening and treatment of strongyloidiasis and
schistosomiasis in migrants (in press). We found no studies providing direct evidence on the effectiveness of
screening for strongyloidiasis or schistosomiasis among migrants, but we identified 28 studies that addressed the
key question along the chain of evidence for screening for schistosomiasis and strongyloidiasis among this
population. Initially, 11 systematic reviews were included, eight focusing on the effectiveness of diagnosis and
treatment of schistosomiasis, and three on the same for strongyloidiasis (292, 301-310). Following a systematic
update of evidence for diagnostic testing for both diseases, ten primary studies were included, seven for
schistosomiasis (311, 312, 313. #331, 314-316) and three for strongyloidiasis (317-319). For the economic
evidence, six studies were included, four for strongyloidiasis and two for schistosomiasis, which consisted of one
systematic review, and five primary studies (three decision-analytic models for economic evaluation and two
costing studies) (320-325).
Strongyloidiasis
Evidence from one systematic review showed that the most effective screening tests for detection of
strongyloidiasis in low intensity/low endemic setting were antibody-detecting serological tests due to their higher
sensitivities compared with conventional parasitological methods (292). Of all conventional methods, agar plate
culture and Baermann methods were the best, with sensitivity/specificity values of 89% (95% CI; 86-92)/100%
(95% CI; 100-100), and 72% (95% CI 67-76)/100% (95% CI; 100-100), respectively (292). The GRADE certainty
of evidence was moderate. They were more specific in comparison to serological techniques (308, 311). However,
these methods are time- and labour-intensive, require skilled personnel and are therefore not recommended as the
first option for public health screening (292).
Serological antibody detection methods exhibited better sensitivity patterns than classical parasitological techniques
(317). Bisoffi et al., reported the accuracy of five serological tests for detection of strongyloidiasis (317). The
sensitivity and specificity values for Luciferase-immunoprecipitation system (LIPS) using 31-kD recombinants
antigen from St. stercoralis (NIE) were 85% (95% CI; 79–92) and 100% [100-100); NIE-ELISA (using the same
antigen) 75% (95% CI 66–83) and 95% (95% CI 91-99); ELISA-IVD – 91%(95% CI 86–96) and 99% (95% CI 97-
100); ELISA-BORDIER 90% (95% CI 84-95) and 98% (95% CI 96-100) and indirect immunofluorescence antibody

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
40
test (IFAT) – 94% (95% CI 90–98) and 92% (95% CI 87-97), respectively (317). However, the certainty of
evidence was low. The disadvantage of current serological tests based on crude antigen (ELISA-IVD and ELISA-
Bordier) are 1) the huge amount of infective larvae required for their production; 2) cross–reactions with other
nematode infections that have been demonstrated mostly in filariasis but also in ascariasis, hydatidosis and also
toxocariasis (292); and 3) the lower sensitivity in immunosuppressed patients (292, 317).
After an effective treatment, the serology has demonstrated a seroreversion or a relevant decline between 3–12
months in a high proportion of infected individuals (326).
Schistosomiasis
The evidence from systematic reviews also showed that the most effective screening tests for detection of
schistosomiasis in low intensity/low endemic setting were antibody-detecting serological tests due to higher
sensitivities compared with conventional parasitological methods (301, 303, 311) such as Kato–Katz (319).
For Schistosoma spp. infections, the most effective screening tests were IgM-ELISA (commercial tests) (327) and
indirect haemagglutination (IHA) tests in non-endemic areas. Point-of-care testing using circulating cathodic
antigen (CCA) tests showed lower specificities and considerable heterogeneity compared with the antibody-
detection methods (301). However, there is ample evidence that a combination of ELISA and Kato–Katz faecal
examinations can improve the detection of Schistosoma spp. in low-intensity settings. In a recent study on the
accuracy of different screening tests for schistosomiasis in African migrants, immunochromatographic IgG/IgM
tests showed the best sensitivity (sensitivity: 96% (95% CI; 91-99), specificity: 83% (95% CI; 77-87)) (328).
Overall, for screening of schistosomiasis and strongyloidiasis, antibody-detecting serological tests appear to be
more sensitive with a good post-test probability of a positive and negative test. However, in the case of
schistosomiasis, the desirable anticipated effects for serological screening are moderate given the variability in
testing methods and species involved. The optimal threshold of prevalence in countries of origin at which to screen
is yet to be determined.
For treatment of schistosomiasis, praziquantel is the drug of choice; treatment with praziquantel significantly
increased parasitological cure with marked reductions in micro-haematuria (304, 305). Ivermectin was more
effective than albendazole in the treatment of strongyloidiasis (310). Moreover, both treatments have a very good
safety profile with few exceptions: ivermectin is contraindicated in patients with a Loa-loa co-infection with high
microfilarial load, and praziquantel should be avoided if there is a possibility of a concomitant neurocysticercosis.
Cost-effectiveness
A preliminary cost study indicated similar costs (of around USD 6–7 per test) for single Kato–Katz stool and urine
tests. Another study comparing screening techniques for parasitic infections showed that eosinophil count may
contribute little to the diagnosis accuracy and generate high costs (325). No studies were available on the cost of
screening tests based on antibody detection in a non-endemic setting. Further economic studies are warranted to
evaluate a test-and-treat strategy for schistosomiasis in non-endemic countries.
In endemic settings, double-dose praziquantel was deemed to be highly cost effective compared with a single dose
(ICER of <USD 500/QALY) for schistosomiasis; the strategy was considered robust to plausible changes in
parameter estimates (320). A few moderate-quality economic studies support a strategy of presumptive treatment
for strongyloidiasis in migrants from high-risk backgrounds. One study showed potential cost savings of universal
treatment with albendazole compared with no intervention (watchful waiting) and universal screening (321).
Presumptive treatment for Strongyloides with ivermectin is cost-effective at a threshold of less than
USD 10 000/QALY across a range of prevalence values. Furthermore, identified economic models with moderate
quality evidence suggested that presumptive treatment with single-dose ivermectin for all immigrants was cost-
effective compared to five days’ treatment with albendazole and to screening (eosinophilia and/or parasitological
techniques only) in the home country (322).
The certainty around several model parameters and feasibility of cost-effective strategies may limit the
transferability of these results to migrants to the EU/EEA for several reasons. First, the calculation of disease
progression to a severe condition and the mortality rate may be underestimated; absence of cost-effective studies
based exclusively on antibody-detecting test (the promoted screening strategy in non-endemic settings); second,
no studies included potential harms of large-scale administration of ivermectin, particularly in migrants coming
from Loa-loa-endemic African countries; and third, ivermectin is not readily available in most endemic countries,
and also not approved by regulatory authorities in the EU/EEA.
Implementation considerations
Screening for schistosomiasis and strongyloidiasis can easily be done with highly sensitive serological antibody-
detecting tests, particularly for strongyloidiasis. For schistosomiasis, given the suboptimal sensitivity in low-intensity
settings, some laboratories prefer to perform two serological tests and consider a case as positive if ‘any’ test is
positive, whereas others undertake a combination of ELISA and Kato–Katz faecal examinations to improve accuracy
for detecting Schistosoma spp. Serological tests are increasingly available in most laboratories. In addition, highly

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
41
effective drugs with excellent tolerability are available for both infections. Screening and treatment is, therefore,
feasible for migrants arriving from endemic countries, irrespective of their prevalence rates.
In the case of immunosuppressed patients with a substantial risk of hyper-infection or disseminated disease, the
recommendation for screening for strongyloidiasis is stronger because the risk of developing severe complications
is substantial (329). Primary care physicians and specialists should be aware of this risk when prescribing
corticosteroids or other immunosuppressants. However, in immunocompromised patients, the sensitivity of
serological tests may be decreased (292); therefore, if serology is negative, parasitological methods should be
added (292). Whenever possible, screening should be performed before the immunosuppression, not only to
preserve the high accuracy of the serological test but also, and more importantly, to minimise the risk of
developing severe complications (329). Finally, and considering the high efficacy and tolerability of ivermectin, it
might be probably worth treating high-risk patients preemptively if an appropriate test (stool culture or serology) is
not available.
It should be noted that both ivermectin and praziquantel are not approved for human use by most national
European medicine agencies. Hence, these drugs are not readily available at the primary care level, but only
supplied at the hospital level (330). It should be also considered that in a particular subgroup of patients,
treatment with ivermectin or praziquantel requires additional complex screening strategies to identify individuals
with loiasis, or neurocysticercosis, for whom the indiscriminate use of these drugs might be deleterious (331-333).
Migrants who are at risk of strongyloidiasis and schistosomiasis face a range of barriers to accessing healthcare
and treatment in the EU/EEA. Addressing these barriers, ensuring the right to healthcare for all, and tailoring
programmes to address the needs of migrant populations are essential to effective screening and treatment
strategies. Systematic reviews did not include data on barriers to screening that are specific to strongyloidiasis and
schistosomiasis. Nevertheless, as with other infectious diseases, barriers are likely to include low risk perception,
limited access to healthcare, particularly for irregular migrants, and socio-economic, cultural and language barriers.
The use of serological tests rather than the routine samples often required when using conventional methods,
together with the availability of treatment, may influence the uptake of schistosomiasis and strongyloidiasis
screening among migrants. In this regard, targeted screening for these infections could take place at the primary
care level and in migrant health clinics, with referral to specialised infectious disease or tropical disease units for
treatment and follow up, until the drugs of choice have become readily available. Physicians responsible for
immunosuppressed patients or patients at risk of immunosuppression should be encouraged to screen for these
infections. This risk, inherent to the underlying disease and/or to the related treatment, concerns an extensive list
of conditions such as neoplasia, transplants, autoimmune and rheumatic diseases, etc. (293).
Ad hoc scientific panel opinion
The scientific panel members were in agreement that screening for schistosomiasis and strongyloidiasis in migrant
populations is an important control strategy that allows for early detection and treatment, reduces individual
morbidity, and prevents onward transmission.
The scientific panel members were asked for their opinion on the evidence relating to: feasibility, acceptability, cost
(resource use), and equity of screening migrants for schistosomiasis and strongyloidiasis. The results of the FACE
survey were as follows:
• Medium level of agreement (73%) that screening for schistosomiasis and strongyloidiasis among migrants is
a priority in the EU/EEA.
• Low level of agreement (21%) that screening for schistosomiasis and strongyloidiasis among migrants is
feasible in the EU/EEA.
• Medium level of agreement (50%) that screening for schistosomiasis and strongyloidiasis among migrants is
acceptable in the EU/EEA.
• Medium level of agreement (57%) that screening for schistosomiasis and strongyloidiasis among migrants is
equitable in the EU/EEA.
The panel anticipated no important variability or uncertainty in patient values and preferences on being screened
and treated for both infections. The panel concluded that the strength of the recommendation was conditional on
the prevalence of schistosomiasis and strongyloidiasis in migrants’ country of origin; the focus should be on
screening of migrants from high-incidence countries. Programmes should address barriers to ensure high uptake of
screening and linkage to care and treatment.

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
42
ECDC assessment
Screening for schistosomiasis and strongyloidiasis in migrant populations is an important control strategy as it
allows for early detection and treatment, probably reduces individual morbidity, and prevents the risk of onward
transmission. Although the evidence-based statements are based on indirect evidence, a very high value is placed
on uncertain but potentially life-preserving benefits of screening, linkage to care, and treatment (334). In this
regard, both infections are potentially severe and chronic; however, the drugs used for treatment of both are
usually well tolerated and safe with few exceptions. Therefore, the health benefits are superior to the potential
harms of intervention. Priority groups include immunosuppressed persons or candidates for immunosuppression. If
the immunosuppression state is already established, screening should be performed with a serological test, plus
parasitological tests.
Figure 6. Countries where schistosomiasis is endemic
Source: IAMAT. World schistosomiasis risk chart 2015. Available from:
https://www.iamat.org/assets/files/World%20Schistosomiasis%20Risk%20Chart_2015.pdf
Note: Public health authorities should consider schistosomiasis screening of migrants from countries marked orange and dark red.
Evidence-based statement (schistosomiasis)
Offer serological screening and treatment (for those found to be positive) to all migrants from countries of high
endemicity in sub-Saharan Africa and focal areas of transmission in Asia, South America, and North Africa (see
Figure 14).
(Certainty of evidence: low)
Evidence-based statement (strongyloidiasis)
Offer serological screening and treatment (for those found to be positive) for strongyloidiasis to all migrants
from countries of high endemicity in Asia, Africa, the Middle East, Oceania and Latin America (see Figure 15).
(Certainty of evidence: low)

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
43
Figure 7. Countries where strongyloidiasis is endemic
So
urce: ECDC expert panel
Note: According to the ECDC expert panel, migrants from countries marked orange should be considered for strongyloidiasis
screening.

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
44
Table 14. Evidence synthesis and guidance for strongyloidiasis and schistosomiasis screening in
migrants
* High (>75%), medium/moderate (50–75%) and low (50%) of ad hoc scientific panel agreed with category.
Evidence gaps and future research needs
Robust population-based studies on schistosomiasis and strongyloidiasis screening among migrants by age group,
migration type, timing of screening and associated cost-effectiveness are required to design the most effective
programmes. High quality surveillance of migrants from highly endemic countries is needed. Also, monitoring any
changes in prevalence between community and holding centres to help guide public health guidance.
Effectiveness
Cost-
effectiveness
Certainty
of
evidence
(GRADE)
FACE survey*
Strength of
recommendation
Implementation
considerations
For the screening of
schistosomiasis and
strongyloidiasis, antibody-
detecting serological tests
identified from included
primary studies were
more sensitive, with very
good post-test probability
of a positive and negative
test (292, 317). For
schistosomiasis, the
desirable anticipated
effects for serological
screening are moderate
given the variations in
testing methods and type
of infection (301,
311).The optimal
threshold of incidence in
countries of origin at
which to screen is yet to
be determined.
There is very little
data on the cost-
effectiveness of
strongyloidiasis
screening in
migrant
populations.
There is no data
on cost-
effectiveness of
schistosomiasis
screening
Limited available
evidence suggests
that presumptive
treatment would
be the most cost-
effective strategy.
However, the
uncertainty
around several
model parameters
and feasibility of
cost-effective
strategies may
limit the
transferability of
these results to
migrants to the
EU/EEA for several
reasons.
Low
The ad hoc
scientific panel
rated the
screening of
strongyloidiasis
and
schistosomiasis
among migrants
in the EU/EEA as
follows:
• Medium
priority
• Low
agreement
that screening
is acceptable
• Moderate
agreement of
feasibility
• Moderate
agreement
that screening
is equitable
Conditional
recommendation
based on country of
origin
In immunosuppressed patients,
with a substantial risk of hyper-
infection or disseminated disease,
the recommendation for
screening is stronger, since the
risk of developing severe
complications is substantial.
Ivermectin and praziquantel are
not readily available, and only
supplied at the hospital level.
Indiscriminate use of these drugs
might be deleterious in patients
with concomitant loiasis or
neurocysticercosis.
Migrants face numerous barriers
to accessing healthcare,
including
socio-
economic, stigma, linguistic
and cultural barriers, and lack of
regular status and insurance; this
may decrease uptake of
strongyloidiasis and
schistosomiasis screening and/or
treatment.
Programmes should address
these barriers to ensure high
uptake of screening and linkage
to care and treatment.

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
45
Recommendations from other national and international guidelines
Table 15. Other international guideline recommendations for parasites for refugee and/or other
migrant populations
Country
When, how and who to test
Australia (9)
Strongyloidiasis:
• Offer blood testing for Strongyloides to all people; if positive, check full blood exam (FBE) for eosinophilia and perform
stool microscopy for ova, cysts and parasite serology to all people.
• Treat with ivermectin. In Loa-loa-endemic countries, rule out loiasis before providing ivermectin.
Schistosomiasis:
• Offer blood testing for schistosomiasis serology if people have lived in/travelled through endemic countries (including
Africa, parts of south-east Asia and the Middle East).
• If tests are positive, treat with praziquantel, perform stool microscopy for ova and perform urine dipstick for haematuria,
and end-urine microscopy for ova if haematuria.
Canada (5)
Strongyloidiasis:
• Screen refugees newly arriving from south-east Asia and Africa with serological tests for Strongyloides spp.
• If positive, treat with ivermectin.
Schistosomiasis:
• Screen refugees newly arriving from Africa with serological tests.
• If positive, treat with praziquantel.
Ireland {#8)
Offer test (ova, cysts and parasites) to symptomatic migrants only, particularly those who have:
• lived or travelled in endemic regions;
• migrated from south-east Asia or sub-Saharan Africa;
• eosinophilia.
Healthcare professionals should also be aware that those with concurrent immunosuppression are at increased risk of
developing disseminated parasitic infections, especially Strongyloides, as this auto-infects and disseminates widely in those
who are immunosuppressed.
Italy (13)
• At initial medical assessment, pay attention to symptoms (diarrhoea, abdominal pain, nausea, vomiting, pruritus,
haematuria) and biochemical markers (eosinophilia) that may be suggestive of parasitosis.
• If symptoms or eosinophilia is present, offer stool examination test for parasitosis.
• Regardless of the presence of symptoms, offer serological tests to all migrants coming from endemic areas (Schistosoma
spp. or Strongyloides). Migrants with a positive serological test should be treated, unless there is already evidence o
f
recent completed treatment.
France (335,
336)
Strongyloidiasis screening for target populations (ELISA + stool examination test for parasitosis):
• Immigrants or refugees from endemic areas, upon arrival.
• All patients originating from, or having lived in, an endemic area prior to commencing immunosuppressive therapy.
Schistosomiasis screening for target populations (serology +/- testing for schistosome eggs in urine or faeces) :
• All migrants from endemic areas.
UK (232,
298)
For refugees, pre-entry:
Helminthic infections:
• Refugees who come from, or reside in, the Middle East, Africa, Asia, Latin America and the Caribbean should be offered
stool test (for ova, cysts and parasites) and serology for strongyloidiasis and schistosomiasis. Refugees should be treated
based on test results.
• Exceptionally, if testing is not available or is logistically impractical and depending on the epidemiological situation,
presumptive treatment with albendazole is indicated during the pre-
departure checks for refugees coming from the Middle
East, Africa, Asia, Latin America and the Caribbean.
− A single dose of albendazole 400 mg for all refugees except pregnant women and children < 2 years of age;
− C
hildren 12 – 23 months of age should have a single dose of albendazole 200 mg.
For migrants, post-arrival:
• The UK has guidance on the investigation of helminth infections for general practices, which should be considered in
migrant patients with unexplained symptoms (especially gastrointestinal) and eosinophilia.
• For migrants from sub-Saharan Africa, screening is recommended for patients with eosinophilia (>0.4 x 10
9
per litre), by
stool microscopy, urine microscopy, strongyloides serology and schistosoma serology
• For migrants from anywhere in the tropics, screening is recommended for patients with eosinophilia (>0.4 x 10
9
per litre),
b
y stool microscopy and strongyloides serology.
• Treatment is according to testing results.
USA (142)
Official guidelines only for refugees and international adoptees. Pre-departure testing or presumptive treatment is
recommended for all categories for strongyloidiasis; testing or presumptive treatment is recommended for schistosomiasis in
all migrants/refugees from sub-Saharan Africa. Testing and/or treatment is generally provided prior to migration. When not
provided pre-departure, post-arrival testing or treatment is recommended.
Refugees from sub-Saharan Africa should receive presumptive therapy for Strongyloides spp. infection with ivermectin if they
resided in, or came from, countries or areas not considered endemic for Loa.
Refugees from sub-Saharan Africa should receive presumptive pre-departure therapy with praziquantel for schistosomiasis

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
46
4.7 Vaccine-preventable diseases
Burden of disease
Control of vaccine-preventable diseases (VPDs) is a priority in the EU/EEA (337). Although national surveillance
systems for VPDs are in place and regular reporting is done, surveillance is incomplete for data on migrants such
as country of birth and time since arrival in the host country and very little information is available on the
occurrence of VPDs among newly arrived migrant populations in the EU/EEA.
Seroprevalence studies have demonstrated suboptimal immunity to VPD among adult and child migrants (29, 338-
345). Some outbreaks of measles and polio in the EU/EEA have been related to under-immunised migrant
populations (346-350), but outbreaks have also occurred in non-migrant populations (30, 351-353). The 2017–
2018 pan-European measles epidemic involved internal EU/EEA migrants moving between countries, so it is
important to also consider this group alongside migrants arriving from outside of the EU/EEA (354) (Figure 13].
WHO data report suboptimal immunisation among the general population worldwide, with global coverage ranging
from 47–85%, depending on the vaccine and the geographical region (355). This includes the EU/EEA, where some
countries have not achieved target vaccine coverage with regard to, for example, first-dose measles (Figure 14).
Among the top ten source countries for migrants to the EU/EEA, the range of age-appropriate (i.e. 2-dose) measles
vaccination coverage ranges from 31–99% (356). Suboptimal immunisation coverage has implications for
maintaining herd immunity in order to minimise outbreaks, which requires seropositivity thresholds of 80–94%
(357, 358). Collective immunity below these thresholds, whether in the native-born population, newly arrived
migrants or a combination of both, carries the inherent risk of disease transmission and outbreak.
A recent cross-sectional survey of EU/EEA countries’ ‘immigrant’ measles vaccination policies found that nine of the
31 countries had no policy and considerable diversity in strategies in the 22 countries that had a policy (359).
Vaccination policies concerning migrants and refugees are heterogenous across the wider WHO European Region
(360). Data on VPDs and vaccination coverage for the EU/EEA demonstrate ongoing transmission in the context of
vaccine coverage below the threshold for herd immunity (361-366). We found no specific data on effective
vaccination implementation strategies for migrants to the EU/EEA.
The evidence review focused on the following VPDs: measles, mumps, rubella, polio, tetanus, diphtheria, pertussis,
and Haemophilus influenzae type b (Hib) disease. Vaccination for hepatitis B is covered in Section 4.4. Varicella and
newer vaccines were not within the scope of this work.
Figure 8. Distribution of measles cases by country, EU/EEA, 1 January–31 December 2017

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
47
Figure 9. Measles vaccination coverage by country, EU/EEA countries, 2017
Summary of evidence
Effectiveness
The systematic review identified ten primary studies (367-376). These studies reported on interventions to increase
vaccine uptake among international migrants (369) and internally displaced people, as both populations face
barriers to vaccination programmes (367, 368, 370-373). Interventions included social mobilisation and community
outreach (368, 370, 371), planned vaccination programmes (369, 373), and education campaigns (367, 368). All
studies were non-randomised and reported an increase in vaccinations. Social mobilisation and outreach
programmes (370-372) appeared to be associated with the greatest increases in vaccination rates.
A study on asylum seekers in Germany reported on a vaccination strategy using some of these approaches (376).
The local public health office informed asylum seekers about relevant VPDs through direct mail, posters, and in
person, and invited them to on-site vaccinations in their housing areas. General practitioners carried out the
vaccinations. Information about vaccination was provided in various languages and by interpreters. Vaccination
certificates were also provided. In areas using this strategy, vaccination rates of 58% were achieved, compared
with 6% in areas that did not offer comparable services. Of 642 vaccinated asylum seekers, 86% were immunised
right in their housing area. There was a particular focus on male adults, among whom an eight-fold increase in
vaccination uptake was recorded. A second European study involved Roma children and women of childbearing age
in a nomadic camp in Rome. As part of a TB outbreak assessment, a monthly vaccination day led to a 56%
coverage of hexavalent vaccines and a 58% coverage of MMR vaccines, a 30% increase in vaccinated subjects
compared with the previous year (368, 370, 371, 373).
Cost-effectiveness
The systematic review identified 26 studies on cost-effective approaches to vaccinations, but only one was focused
on migrants (377). It compared pre-vaccination serotesting with presumptive immunisation for polio, diphtheria,
and tetanus in internationally adopted and immigrant infants to the US (377). It showed that, compared with
presumptive immunisation, pre-vaccination serotesting for polio increased the cost per patient from USD 57 to
USD 62 and decreased the percentage of patients protected against polio from 95.3% to 94.0%. Presumptive
immunisation was more effective and less expensive than pre-vaccination serotesting when seroprevalence was
<69%. Presumptive immunisation was the preferred method unless vaccination compliance was extremely high
(>96% completion rate) (377). Results for diphtheria, tetanus and pertussis (DTaP) were less definitive. Pre-
vaccination serotesting for diphtheria and tetanus increased the cost per patient from USD 62 to USD 119 and
increased the percentage of patients protected against both diphtheria and tetanus from 91.5% to 92.3% (377).

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
48
Presumptive immunisation was the preferred strategy with an ICER of USD 7 148 per infant protected in
populations with poor vaccine compliance (where >80% of patients did not complete the full catch-up vaccine
series), or populations with low seroprevalence (<51%) of antibodies to diphtheria and tetanus (377).
Two US studies that were published after the systematic review was performed, examined different costs
associated with pre-departure vaccinations, one in the context of a response to an outbreak (378) and one
evaluating the US Vaccination Program for US-bound Refugees (VPR) (379). The first study showed that pre-
departure vaccination of all US-bound refugees would not only improve health and reduce importations of VPD, but
would also be cost saving when considering all the resources required for response to outbreaks (378). The second
study demonstrated that – compared with post-arrival vaccinations – the initiation of the pre-departure VPR where
the refugees received one or two doses of selected vaccines before departure and completed the series after
arrival, demonstrated a net savings per person of USD 225.93 (a 29% decrease in vaccination costs). The cost
savings were sensitive to different variables, but demonstrated cost savings across all estimates.
Implementation considerations
Engaging migrant populations in preventive health services remains a challenge in view of the barriers they face in
accessing healthcare (177, 380). A recent consensus statement on access to health services in the EU/EEA by
IOM’s EQUI-HEALTH project (381) highlights the discrepancies in entitlements to statutory health services for
migrants; irregular migrants often have highly restrictive access. Barriers to immunisations for migrants include:
use of traditional healthcare (382), socio-economic status (382), language (383), distance to immunisation service
(383, 384), continued migration (384), fear of arrest (384), necessity of work (384), lack of vaccination knowledge
(383, 385, 386), cost (386) and lack of healthcare provider recommendation (387). Well-informed migrants
routinely accept vaccination, sometimes at a rate higher than the native population (388).
Bundling of primary care services for migrants may prevent further barriers to vaccination, diagnosis, and care.
Clinicians should assess immunisation documentation and provide migrants with documentation of vaccines
administered. Social mobilisation appears promising to increase vaccination coverage in migrant populations (368,
370, 371). Multiple opportunities for vaccinations occur at different points in the migration trajectory. Information
regarding immunisation should be available in multiple languages, particularly those most commonly spoken by
arriving migrants.
Italy, Ireland, Australia, Canada the UK and the US have all published migrant-specific VPD guidelines (see Table
17), yet concerns have been raised as to the extent such guidelines are implemented in practice and the need to
consider wider groups of migrants beyond refugees and asylum seekers in catch-up vaccination programmes (360,
389). The WHO, UNHCR and UNICEF have published a joint statement on general principles on vaccination of
refugees, asylum-seekers and migrants in the WHO European Region (390). In 2015, ECDC suggested vaccinations
for newly arriving migrants be offered in accordance with the national immunisation guidelines of the host country
(61). These migrant guidelines recommend assessing the immunisation record of the migrants and not pursuing
serology testing. WHO has published a framework for decision-making about vaccinations for migrants in acute
humanitarian emergencies. This framework looks at epidemiological risk assessments, vaccine characteristics, and
contextual factors in a three-step process of decision-making (390).
Ad hoc scientific panel opinion
The ad hoc scientific panel members were in agreement that vaccination in migrant populations is important in
terms of VPD control and equity. The panel concluded that the strength of the recommendation was strong for
child and adolescent migrants and conditional on health system resources for adult migrants.
The scientific panel members were asked for their opinion on the evidence relating to feasibility, acceptability, cost
(resource use), and equity of vaccinations among migrants. The results of the FACE survey showed the following:
• High level of agreement (80%) that providing vaccinations to migrants is a priority in the EU/EEA.
• High level of agreement (93%) that providing vaccinations to migrants is feasible in the EU/EEA.
• High level of agreement (100%) that providing vaccinations to migrants is acceptable in the EU/EEA.
• High level of agreement (100%) that providing vaccinations to migrants is equitable in the EU/EEA.
The ad hoc scientific panel agreed that there are additional considerations to take into account when proposing
vaccination of adult migrants. Healthcare accessibility was considered by all as a critical issue, given the barriers
that migrants often face. Integrating migrants into primary care and public health programmes would increase
feasibility. The panel agreed that it is important to ensure that migrant children and adults receive vaccination
coverage similar to that of EU/EEA citizens. However, it also recognises that immunisation of migrants increases the
complexity of vaccination programmes because of the need to address language and cultural differences.

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
49
ECDC assessment
Control of VPDs is an important priority for the EU/EEA. Migrants have been shown to have suboptimal immunity
against VPDs and outbreaks of VPDs have occurred in migrant populations living in the EU/EEA. All migrant
children and adolescents should be vaccinated in accordance with the host countries’ vaccine schedules to support
health equity. Migrant adults without prior vaccination records should be vaccinated in accordance with the host
country vaccine schedule. In the case of migrant children and/or incomplete records, age-appropriate catch-up
schedules are recommended. MMR and DTaP-IPV-Hib vaccines should be prioritised for children and adolescents.
In adults without an immunisation record or with incomplete immunisations, MMR and diphtheria, pertussis,
tetanus immunisation is recommended. Migrants face many barriers to accessing healthcare that can lead to low
uptake of vaccinations. Social mobilisation and culturally and linguistically appropriate community outreach paired
with planned vaccination programmes have been shown to increase vaccine uptake among migrants internationally
and in the European context; more evaluation to identify effective implementation strategies in the EU/EEA is
required.
Evidence-based statement 1
Offer vaccination against measles/mumps/rubella (MMR) to all migrant children/adolescents without
immunisation records as a priority.
(Certainty of evidence: low)
Evidence-based statement 2
Offer vaccination to all migrant adults without immunisation records with either one dose of MMR or in
accordance with the MMR immunisation schedule of the host country.
(Certainty of evidence: very low)
Evidence-based statement 3
Offer vaccination against diphtheria, tetanus, pertussis, polio and HiB (DTaP-IPV-Hib) to all migrant children/and
adolescents without immunisation records as a priority.
(Certainty of evidence: low)
Evidence-based statement 4
Offer vaccination to all adult migrants without immunisation records in accordance with the immunisation
schedule of the host country. If this is not possible, adult migrants should be given a primary series of
diphtheria, tetanus, and polio vaccines.
(Certainty of evidence: very low).
For the evidence-based statement on hepatitis B vaccination, please see Section 4.4.

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
50
Table 16. Evidence synthesis and guidance for VPDs in migrant populations
Effective
implementation
strategies
Cost-
effectiveness
Certainty
of
evidence
(GRADE)
FACE survey*
Strength of
recommendation
Implementation
considerations
All guidelines
recommend assessing
a migrant’s
immunisation record
and not pursuing
serology testing.
Vaccination is to be
offered in accordance
with the national
immunisation
guidelines of the host
country.
Social mobilisation
and outreach
programmes appear
to be associated with
the most significant
increases in
vaccination rates
(370-372).
There are very
little data on the
cost-effectiveness
of vaccination
strategies in
migrant
populations.
Serological testing
was less cost-
effective than
presumptive
immunisation of
internationally
adopted children.
Pre-departure
vaccination of
refugees was cost-
saving and
decreased vaccine-
preventable
diseases.
Very low to
moderate.
The ad hoc
scientific panel
rated
immunisation
against VPDs
among migrants in
the EU/EEA as
follows:
• High
agreement
around priority
• High
agreement of
acceptability
• High
agreement
around
feasibility
• High
agreement that
vaccination
migrants is
equitable
Strong
recommendation for
children/adolescents.
Conditional
recommendation for
adults.
All migrant children/
adolescents should be
vaccinated according to the
host country’s vaccine
schedules.
Adult migrants without
vaccination records should be
offered catch-up vaccination in
accordance with the host
country vaccine schedule.
Measles/mumps/rubella (MMR)
and diphtheria, tetanus and
polio vaccines should be
prioritised.
Provide migrants with
documentation of vaccines
administered to prevent
vaccination duplication.
Social mobilisation could be
used to increase vaccination
coverage in migrant
populations. Primary healthcare
interactions remain an
important opportunity for
assessing vaccination status
and offering vaccinations.
Information regarding
immunisation should be
available in multiple languages,
particularly those most
commonly spoken by newly
arriving migrants.
* High (>75%), medium (50–75%) and low (50%) of ad hoc panel agreed with category
Evidence gaps and future research needs
National immunisation guidelines, plans and programmes should include a specific focus on migrants, considering
both internal migrants within the EU/EEA and external migrants to the EU/EEA. Robust surveillance data on VPDs
and vaccine coverage in migrant populations by age group, migration type, source country, and duration of
presence in the EU/EEA are required to design the most effective programmes (391). This will require
standardisation of migrant definitions and variables. Evidence on the effectiveness and cost-effectiveness of
different immunisation strategies for migrants is required as is specific research on vaccination uptake and
immunisation coverage in adults vs. children to inform prioritisation and guidelines. The optimal approach to
document immunisations and share immunisation data concerning mobile populations across jurisdictions to avoid
vaccination duplication is an understudied area (392).
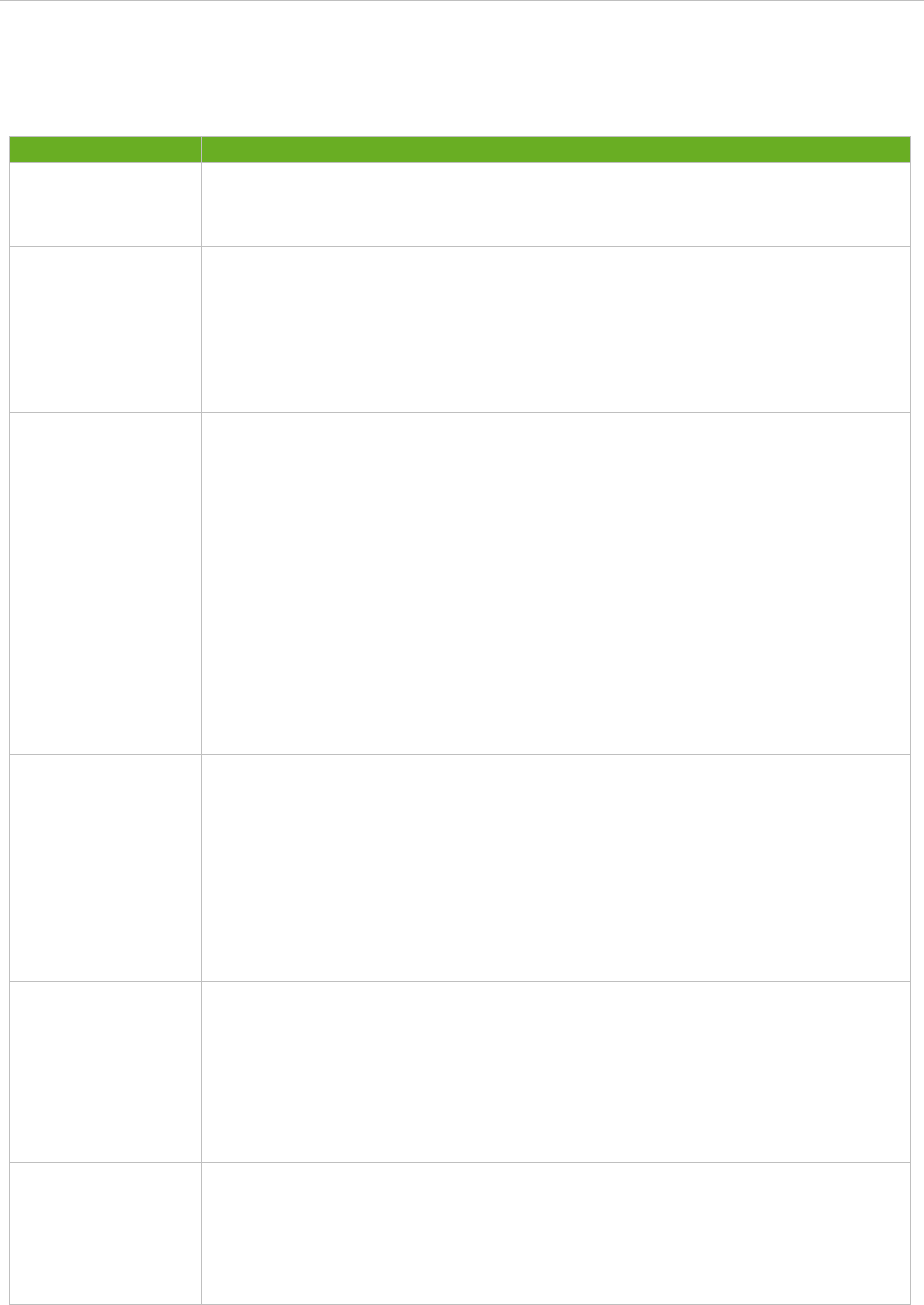
SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
51
Recommendations from other national and international guidelines
Table 17. International guideline VPD recommendations for refugees and/or other migrant
populations
Country
How and who to vaccinate
Australia (9)
• Assess availability of immunisation records; plan vaccination based on age.
• Provide catch-up immunisation so people from refugee-like backgrounds are immunised
equivalent to an Australian-born person of the same age.
• Full catch-up if records are not available
Canada (5)
Measles, mumps and rubella
• Vaccinate all adult immigrants without immunisation records using one dose of measles–mumps–
rubella vaccine.
Diphtheria, pertussis, tetanus, polio
• Vaccinate all adult immigrants without immunisation records using a primary series of tetanus,
diphtheria and inactivated polio vaccine (three doses), the first of which should include a cellular
pertussis vaccine.
Ireland (8)
Assess all migrants for previous measles vaccination.
MMR
All migrants without documented evidence of previous measles vaccination should be offered MMR
vaccination as follows:
• All children in accordance with the routine childhood immunisation schedule at 12 months and 4–
5 years of age (2 doses)
• All others according to the ‘late entrants catch-up schedule’ for children and adults, as follows:
− 12 months to 4 years, 1 dose MMR, 2nd dose at 4–5 years of age
− 4 years to <18 years of age, 2 doses MMR at one month interval
− Adults aged 18 years and older, 2 doses MMR at one month interval
DTaP-IPV
• Vaccinate all adult immigrants without immunisation records using a primary series of tetanus,
diphtheria and inactivated polio vaccine (three doses), the first of which should include acellular
pertussis vaccine.
• Vaccinate all immigrant children with missing or uncertain vaccination records using age-
appropriate vaccination for diphtheria, pertussis, tetanus and polio.
Italy (13, 393)
Primary prevention interventions (vaccinations) as well as secondary prevention interventions are
recommended in the second reception phase.
Children (0–14 years) never vaccinated or with uncertain or unknown vaccination status: vaccinations
in accordance with the national schedule, depending on age.
Adults with uncertain or no vaccination history:
• polio
• measles, mumps, rubella, chickenpox; excluding pregnant women
• diphtheria, tetanus, pertussis, HBV for the entire adult population screened in accordance with
guideline recommendations (migrants from HBV incidence of HBsAg >2%, migrants with ris
k
factors, and pregnant women) and negative for serological markers.
UK (232, 233)
• The UK offers vaccinations in line with the national immunisation schedule to any migrant whose
immunisation status is uncertain or incomplete, in accordance with guidance for individuals with
uncertain or incomplete immunisation status.
• All migrants are eligible for vaccines through the National Immunisation Programme and can
access immunisation services the same way as the rest of the population.
• Refugees who are to be resettled in the UK through a formal refugee resettlement scheme ar
e
o
ffered vaccination pre-departure, in line with the national immunisation schedul
e.
• Asylum seekers in initial accommodation centres in the UK are offered vaccination as part of their
initial health assessment.
USA (394)
• Immigrants are required to show proof that they have received certain vaccines prior to arrival.
• If an applicant does not have proof of having received the required vaccines, the law states that
the initial doses vaccines must be given at the time of the medical examination.
•
Refugees and international adoptees are exempt from this requirement, however they are offered
1–3 doses of each vaccine series (394).
• Following arrival, all immigrants are recommended that they have their vaccinations updated in
accordance with national guidelines (ACIP) (395, 396).

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
52
5. Implications for public health practice and
research
5.1 Public health practice
This ECDC guidance provides evidence-based assessments on public health interventions – vaccination, screening
and linkage to treatment and care – in order to decrease the burden of disease among migrant populations in the
EU/EEA and promote health in these population groups. It addresses infectious diseases that disproportionately
affect migrants and focuses on interventions for newly arrived migrants to the EU/EEA. The guidance is intended to
inform public health policy and programmes and aims to improve implementation and service delivery; it does not
provide detailed clinical recommendations.
The evidence cited in this document is overwhelmingly based on data and lessons from high-risk non-migrant
populations and approaches used in low- and middle-income countries. Further input was received through the
views of a range of experts. Although the quality of some of the evidence for effectiveness and cost-effectiveness
is low, this guidance identifies potential approaches to improve health outcomes for migrants in the EU/EEA.
Available evidence suggests that the screening of migrants is likely to be both effective and cost-effective for active
TB, LTBI, HIV, HCV, HBV, strongyloidiasis and schistosomiasis. There are clear benefits to be derived from enrolling
migrants in vaccination programmes and ensuring catch-up vaccinations. Screening for priority infectious diseases
is, however, conditional on the prevalence of the disease in a migrant’s country of origin.
5.2 Linkage to care
Although identifying infectious diseases early through testing is a critical clinical and public health intervention, it is
only one element of the care pathway (26). Integral to the development of this guidance is an understanding of
the importance of, and interventions for, each element of the care pathway, from access to appropriate health
services to testing/screening and adherence to/completion of treatment.
Experience relating to a range of infections shows that post-testing losses occur at all stages of the clinical care
pathway. These include failure to get results after testing, failure to attend specialist services to commence
treatment, and failure to complete or adhere to treatment (124, 397-400). Although data for migrants are less
clear (401), the same principle of minimising dropout across the cascade following screening/diagnostic testing
applies.
Dropouts at each stage of the care pathway can be due to a number of personal and system-level barriers that
migrants may face in accessing statutory health/appropriate health services on arrival and after, for example due to
the lack of clarity about the organisation and financing of care, compounded by linguistic and cultural barriers
(402-404). Many vulnerable migrant groups are not entitled to free statutory healthcare on arrival, which will
undoubtedly impact on uptake of screening and attendance at specialist services (404). Additional concerns for
new migrants to European countries include competing psycho-social priorities such as housing, employment,
concerns about family reunion, mental health issues and chronic diseases. These problems not only interfere with
testing, but also have the potential to increase the risks or consequences of infectious diseases. This synergistic
interaction linked to socially disadvantaged circumstances, known as syndemics, calls for an integrated approach of
public health and primary care, addressing biomedical as well as psychosocial problems (405).
Therefore, it is important that ease of access, making health services responsive, and engaging migrant
communities is considered at an early stage when developing clinical pathways relating to screening for infection
and appropriate vaccination (406). Engagement includes providing the necessary information and tailoring services
to the needs and possibilities of the migrants involved (104, 407, 408). While this early work may seem less
important, it likely sets in motion the basis for future community engagement and the co-development of services,
which are critical to reaching individuals from often marginalised and neglected communities (409).
It is also important to consider the way in which screening/testing is framed and offered, as this can have an
impact on whether individuals from migrant communities accept testing, how they view the results, and whether
they attend for follow-up care and complete treatment. Testing is only one element of the care pathway and,
without follow-up case and treatment, has limited individual or public health benefit. A decision to test should
equate to an intention to refer for assessment and, if required, treatment. Particular attention, therefore, needs to
be given to the linkage between testing and referral and specialist care when designing programmes and services
for migrants and providing education and information to migrants and health professionals. Ease of access and
responsiveness can be enhanced by offering integrated services that consider multiple infections, rather than just
screening for TB, for example. This will require working more closely with migrant communities to ascertain their
view and concerns, but certain elements should be incorporated including (410):

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
53
• Collaboration between public health, primary care and specialist care in order to ensure continuity of care
tailored to all the needs of the person involved.
• Single point-of-referral to a migrant-friendly clinical service with culturally competent staff who can manage
infectious diseases and other health needs alongside interpreters and other support services to enhance
treatment adherence and completion.
• Robust data collection to facilitate sharing of best practice with respect to linkage to care and treatment
completion for migrants with infectious diseases.
5.3 Research gaps
The process of developing this guidance has highlighted gaps in knowledge concerning infectious disease
interventions targeting migrant populations.
Research is needed to provide strong evidence on how best to deliver screening and vaccination to migrant
populations, challenges around diagnosis and treatment, and on the impact of interventions. More robust data are
needed on the acceptability, effectiveness, and cost-effectiveness of screening and vaccination programmes
targeting migrants. Large linked datasets studies or multi-country and multi-ethnic group studies are needed to
improve the precision of estimates of disease, morbidity, and mortality. More research, including community-based
participatory action research, is also needed on the determinants of health in migrant populations and migrant
community perspectives on screening and vaccination. Research into multiple disease screening (i.e. screening
concomitantly for HIV, TB and hepatitis and intestinal parasites when indicated) (93) and roles for screening in
community-based primary healthcare services should be a priority.
Furthermore, countries should consider research and innovations in public policy and migration, new forms of
EU/EEA cooperation and governance, programmes to empower migrants and technology to support integration and
communications.

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
54
6. Next steps
Public health programmes have an important role in improving the health and social determinants of health for
newly arriving migrant populations to the EU/EEA. This ECDC guidance provides the evidence base to enable
EU/EEA Members States to develop and adapt their own public health and clinical guidance on screening and
vaccination for newly arrived migrant populations.
Public health programmes need to target screening and vaccination programmes towards high-risk migrant
populations and take steps to increase uptake of screening and vaccination, to improve linkage to care and
treatment, and to improve retention across the cascade of care for infectious diseases. Health programmes and
services will need to adapt their approaches to optimise public health benefits and meet the needs of migrant
populations, including providing culturally and linguistically sensitive services and offering integrated screening,
vaccination and care services. For example, using rapid HIV tests can dramatically improve uptake of testing;
multiple test approaches are often preferred by migrants who may require serology testing for multiple infectious
diseases.
Since the majority of preventive and curative healthcare for migrants is provided by community-based primary care
services, there is a need to improve health professionals’ awareness and skills with respect to migrant health needs
and ensure delivery of non-stigmatising services that respect privacy and confidentiality. Community engagement,
through outreach and community-based care, is also critical to improving awareness and uptake among migrant
populations. Community-based care can improve trust and ease of access to screening and vaccination services.
There is an opportunity to learn from the experience of EU/EEA countries that are implementing effective
programmes to reach newly arrived migrants through approaches that include culturally sensitive health promotion,
use of interpreters, training of community-based primary care professionals, and collaboration with public health
and migrant community coalitions.
The guidelines also highlight the need to address the various socio-economic, cultural, legal and other barriers that
limit access to, and uptake of, healthcare services. Particular attention needs to be given to ensuring that economic
barriers do not inhibit or prohibit migrants from seeking or obtaining vaccination, screening and treatment for
infectious diseases.
Better understanding is needed of migrant perceptions about infectious diseases, disease susceptibility, benefits of
screening, testing and vaccination, and the acceptability and accessibility of healthcare services, as well as better
monitoring of uptake of services. In addition, improvements in surveillance are required to increase the
completeness and quality of data and inform more accurate estimates of disease prevalence, morbidity and
mortality among migrant populations.
This guidance will be reviewed five years after publication to determine whether it requires updating in light of new
evidence and developments in migrant health and migrant demographics in the EU/EEA.

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
55
References
1. Preamble to the Constitution of World Health Organization, (adopted 1946, entered into force 7 April 1948). Available at:
http://apps.who.int/gb/bd/PDF/bd47/EN/constitution-en.pdf
.
2. United Nations. United Nations Statistics Division - Demographic and Social Statistics. 2017. Available at:
https://unstats.un.org/unsd/demographic-social/index.cshtml.
3. Convention relating to the Status of Refugees United Nations Conference of Plenipotentiaries on Status of Refugees and
Stateless Persons; 1950. Available at: https://www.ohchr.org/EN/ProfessionalInterest/Pages/StatusOfRefugees.aspx
.
4. International Organization for Migration. World Migration Report 2015. Migrants and Cities: New Partnerships to Manage
Mobility 2015. Available at: https://www.iom.int/world-migration-report-2015
.
5. Pottie K, Greenaway C, Feightner J, Welch V, Swinkels H, Rashid M, et al. Evidence-based clinical guidelines for immigrants
and refugees. CMAJ. 2011;183:E824-E925.
6. Gushulak BD, Pottie K, Hatcher Roberts J, Torres S, DesMeules M, Canadian Collaboration for I, et al. Migration and health
in Canada: health in the global village. CMAJ. 2011;183(12):E952-8.
7. Thiel de Bocanegra H, Carter-Pokras O, Ingleby JD, Pottie K, Tchangalova N, Allen SI, et al. Addressing refugee health
through evidence-based policies: a case study. Annals of Epidemiology. 2017.
8. Health Protection Surveillance C. Infectious Disease Assessment for Migrants. Dublin, Ireland: 2015. Available at:
https://www.hpsc.ie/a-z/specificpopulations/migrants/guidance/File,14742,en.pdf
.
9. Chaves NJ, Paxton G, Biggs BA, Thambiran A, Smith M, Williams J, et al. on behalf of the Australasian Society for Infectious
Diseases and Refugee Health Network of Australia Guidelines writing group. Recommendations for comprehensive post-
arrival health assessment for people from refugee-like backgrounds. Australasian Society for Infectious Diseases Inc., 2016
.
A
vailable at: https://www.asid.net.au/documents/item/1225
.
10. US Centers for Disease Prevention and Control (US CDC). Immigrant and Refugee Health. Guidelines for the U.S. Domestic
Medical Examination for Newly Arriving Refugees 2018 [cited 2018]. Available at:
https://www.cdc.gov/immigrantrefugeehealth/guidelines/domestic/domestic-guidelines.html
.
11. Public Health England. Assessing new patients from overseas: migrant health guide. Public Health England, 2014 31 July
2014. Available at: https://www.gov.uk/guidance/assessing-new-patients-from-overseas-migrant-health-guide#history
.
12. Pre-entry health assessments for UK-bound refugees. Home Office; Public Health England; International Organization for
Migration, 2017 August 2017. Available at: https://
www.england.nhs.uk/south/wp-
content/uploads/sites/6/2014/06/refugee-health-protocal.pdf.
13. INMP, SIMM controlli alla frontiera. La frontiera dei controlli. Controlli sanitari all’arrivo e percorsi di tutela per i migranti
o
spiti nei centri di accoglienza. Sistema Nazionale per le Linee-guida. June 2017. Available at:
http://www.inmp.it/lg/LG_Migranti-integrata.pdf
.
14. Mipex. Migrant Integration Policy Index. Brussels: Migration Policy Group in collaboration with the Barcelona Centre for
International Affairs (CIDOB); 2015.
15. Dara M, de Colombani P, Petrova-Benedict R, Centis R, Zellweger J-P, Sandgren A, et al. Minimum package for cross-borde
r
T
B control and care in the WHO European Region: a Wolfheze consensus statement. The European Respiratory Journa
l.
2
012;40(5):1081-90.
16. Heldal E, Kuyvenhoven JV, Wares F, Migliori GB, Ditiu L, Fernandez de la Hoz K, et al. Diagnosis and treatment of
t
uberculosis in undocumented migrants in low- or intermediate-incidence countries. The International Journal o
f
T
uberculosis and Lung Disease: the official journal of the International Union against Tuberculosis and Lung Disease
.
2
008;12(8):878-88.
17. European Centre for Disease Prevention and Control Asessing the burden of key infectious diseases affecting migrant
populations in the EU/EEA. Stockholm: ECDC; 2014. Available at:
https://ecdc.europa.eu/sites/portal/files/media/en/publications/Publications/assessing-burden-disease-migrant-
populations.pdf.
18. Pottie K, Mayhew AD, Morton RL, Greenaway C, Akl EA, Rahman P, et al. Prevention and assessment of infectious diseases
among children and adult migrants arriving to the European Union/European Economic Association: a protocol for a suite o
f
systematic reviews for public health and health systems. BMJ Open. 2017;7(9).
19. Greenaway C, Pareek M, Abou Chakra CN, Walji M, Makarenko I, Alabdulkarim B, et al. The effectiveness and cost-
effectiveness of screening for active tuberculosis among migrants in the EU/EEA: a systematic review. Euro Surveil
l.
2
018;23(14).
20. Greenaway C, Pareek M, Abou Chakra CN, Walji M, Makarenko I, Alabdulkarim B, et al. The effectiveness and cost-
effectiveness of screening for latent tuberculosis among migrants in the EU/EEA: a systematic review. Euro Surveill.
2
018;23(14).
21. Pottie K, Lotfi T, Kilzar L, Howeiss P, Rizk N, Akl E, et al. The Effectiveness and Cost-Effectiveness of Screening for HIV in
Migrants in the EU/EEA: A Systematic Review. Int J Environ Res Public Health. 2018;15(8):1700.
22. Myran D, Morton R, Biggs B-A, Veldhuijzen I, Castelli F, Tran A, et al. The Effectiveness and Cost-Effectiveness of Screening
for and Vaccination Against Hepatitis B Virus among Migrants in the EU/EEA: A Systematic Review. Int J Environ Res Public
Health. 2018;15(9):1898.
23. Greenaway C, Makarenko I, Abou Chakra C, Alabdulkarim B, Christensen R, Palayew A, et al. The Effectiveness and Cost-
Effectiveness of Hepatitis C Screening for Migrants in the EU/EEA: A Systematic Review. Int J Environ Res Public Health
.
2
018;15(9):2013.
24. Hui C DJ, Morton R, et al. Interventions to Improve Vaccine Uptake an Cost-Effectiveness of Vaccination Strategies in Newly
Arrived Migrants in the EU/EEA: A Systematic Review. It J Environ Res Pub Health. 2018;15:2065.
25. Driedger M, Mayhew A, Welch V, Agbata E, Gruner D, Greenaway C, et al. Accessibility and Acceptability of Infectious
Disease Interventions Among Migrants in the EU/EEA: A CERQual Systematic Review. Int J Environ Res Public Health
.
2
018;15(11):2329. https://www.mdpi.com/1660-4601/15/11/2329/htm
.
26. Pareek M, Noori T, Hargreaves S, van den Muijsenbergh M. Linkage to Care Is Important and Necessary When Identifying
Infections in Migrants. Int J Environ Res Public Health. 2018;15(7):1550.

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
56
27. European Centre for Disease Prevention and Control. Epidemiological assessment of hepatitis B and C among migrants in
the EU/EEA. Stockhlom: ECDC, 2016. Available at:
https://ecdc.europa.eu/sites/portal/files/media/en/publications/Publications/epidemiological-assessment-hepatitis-B-and-C-
among-migrants-EU-EEA.pdf.
28. Gushulak B, Pace P, Weekers J. Poverty and social exclusion in the WHO European Region: health systems respond. In:
Koller T, editor: World Health Organization; 2010. p. 257-81.
29. Mipatrini D, Stefanelli P, Severoni S, Rezza G. Vaccinations in migrants and refugees: a challenge for European health
systems. A systematic review of current scientific evidence. Pathogens and Global Health. 2017;111(2):59-68.
30. Grammens T, Maes V, Hutse V, Laisnez V, Schirvel C, Trémérie JM, et al. Different measles outbreaks in Belgium, January
to June 2016–a challenge for public health. Eurosurveillance. 2016;21(32).
31. Tavares AM, Fronteira I, Couto I, Machado D, Viveiros M, Abecasis AB, et al. HIV and tuberculosis co-infection among
migrants in Europe: A systematic review on the prevalence, incidence and mortality. PloS one. 2017;12(9):e0185526.
32. Stronks K, Snijder MB, Peters RJG, Prins M, Schene AH, Zwinderman AH. Unravelling the impact of ethnicity on health in
Europe: the HELIUS study. BMC Public Health. 2013;13:402.
33. Tankimovich M. Barriers to and interventions for improved tuberculosis detection and treatment among homeless and
immigrant populations: a literature review. Journal of Community Health Nursing. 2013;30(2):83-95.
34. Norredam M, Agyemang C, Hoejbjerg Hansen OK, Petersen JH, Byberg S, Krasnik A, et al. Duration of residence and
disease occurrence among refugees and family reunited immigrants: test of the ‘healthy migrant effect’ hypothesis. Tropica
l
M
edicine & International Health. 2014;19(8):958-67.
35. Padilla B, Miguel JP. Health and Migration in the European Union: Better Health for All in an Inclusive Society: Chapter 1:
Health and Migration in the European Union: Building a Shared Vision for Action. 2009. p. 15-22. Available at:
http://www.academia.edu/3757255/Health_and_migration_in_the_European_Union_Good_practices
.
36. Semenza JC, Carrillo-Santisteve P, Zeller H, Sandgren A, van der Werf MJ, Severi E, et al. Public health needs of migrants, refugees
and asylum seekers in Europe, 2015: Infectious disease aspects. European Journal of Public Health. 2016;26(3):372-3.
37. Migration and health: a complex relation. The Lancet. 2006;368(9541):1039.
38. Eurostat. Population statistics. Migrant population. Eurostat migr_pop3ctb. Available at:
http://appsso.eurostat.ec.europa.eu/nui/show.do?dataset=migr_pop3ctb&lang=en%20
.
39. Eurostat. Population statistics. Migrant population. Eurostat migr_resfirst. Available at:
http://appsso.eurostat.ec.europa.eu/nui/show.do?dataset=migr_resfirst&lang=el
.
40. Eurostat. Population statistics. Migrant population. Eurostat migr_resfirst, migr_resoth. Available at: http://ec.europa.eu/eurostat/statistics-
explained/index.php/Residence_permits_statistics#First_residence_permits_by_reason.
41. Frontex. Data from Frontex. Available at: https://frontex.europa.eu/assets/Migratory_routes/Detections_of_IBC_2018_05_07.xlsx.
42. Eurostat. Population statistics. Migrant population. Eurostat migr_asyappctza. . Available at:
http://appsso.eurostat.ec.europa.eu/nui/show.do?dataset=migr_asyappctza&lang=EN
.
43. European Parliament. EU-Turkey Statement and Action Plan, 2016. Available at: http://wwweuroparleuropaeu/legislative-
train/theme-towards-a-new-policy-on-migration/file-eu-turkey-statement-action-plan.
44. Eurostat. Statistics explained. Asylum statistics. Eurostat tps00192, tps00193. Available at:
http://ec.europa.eu/eurostat/statistics-explained/index.php?title=Asylum_statistics
.
45. Eurostat. Statistics explained. Asylum statistics. Eurostat migr_asydcfsta, tps00193. Available at:
http://ec.europa.eu/eurostat/statistics-explained/index.php?title=Asylum_statistics
.
46. European Parliament. EU Migrant Crisis: facts and figures. 2017. Available at:
http://wwweuroparleuropaeu/news/en/headlines/society/20170629STO78630/eu-migrant-crisis-facts-and-figures
.
47. Eurostat. Population by age group, sex and citizenship. Eurostat migr_pop1ctz. Available at:
http://appsso.eurostat.ec.europa.eu/nui/show.do?wai=true&dataset=migr_pop1ctz
.
48. Committee on Economic Social and Cultural Rights. General Comments No. 14: The Right to the Highest Attainable
Standard of Health (Art. 12). 2009. Available from:
https://tbinternet.ohchr.org/_layouts/treatybodyexternal/TBSearch.aspx?Lang=en&TreatyID=9&DocTypeID=11
49. United Nations. Convention on the Rights of the Child, Nov. 20, 1989, 28 I.L.M. 1448 (1989), corrected at 29 I.L.M. 1340
(1990) (entered into force 2 September 1990), Article 24(2)(d). 1989.
50. European Observatory on Health Systems and Policies. Children’s universal right to healthcare in the EU: compliance with
the UNCRC. July 2017. Available at: http://www.euro.who.int/__data/assets/pdf_file/0006/357486/EH_v23n4.pdf
.
51. United Nations. Convention on the Elimination of All Forms of Discrimination Against Women. Dec. 18, 1979, 1249 U.N.T.S.
13,
19 ILM. 33 (entered into force 3 September 1981), Article 12(2).
52. European Union. Charter of Fundamental Rights to the European Union, Article 35. Official Journal of the European
Communities. 2012/C(364/01). Available at: European Union. Charter of Fundamental Rights to the European Union, Article
35
.
Official Journal of the European Communities.2012/C(364/01).
53. European Union Agency for Fundamental Rights. Fundamental Rights Report 2016. Available at:
http://fra.europa.eu/en/publication/2016/fundamental-rights-report-2016
.
54. Amets Suess IRP, Ainhoa Ruiz Azarola, Joan Carles March Cerdà. The right of access to healthcare for undocumented migrants: a
revision of comparative analysis in the European context. European Journal of Public Health. 2014;24(5):712-20.
55. European Centre for Disease Prevention and Control. HIV and laws and policies in Europe: Monitoring implementation o
f
t
he Dublin Declaration on partnership to fight HIV/AIDS in Europe and Central Asia. 2017. Available at:
https://ecdc.europa.eu/en/publications-data/evidence-brief-hiv-and-laws-and-policies-europe.
56. Medecins du Monde. 2017 Observatory report – Falling through the cracks: the failure of universal coverage in Europe.
20
17. Available at: https://
www.medecinsdumonde.org/en/actualites/publications/2017/11/08/falling-through-cracks-
failure-universal-healthcare-coverage-europe.
57. Hargreaves S, Rustage K, Nellums LB, Powis Jaynaide, Milburn J, Severoni S, et al. What constitutes an effective and
efficient package of services for the prevention, diagnosis, treatment and care of tuberculosis among refugees and
migrants in the WHO European Region? Themed issues on migration and health, VIII. Health Evidence Network Synthesis
Report 56. Copenhagen: WHO Regional Office for Europe, 2018. Available at:
http://www.euro.who.int/__data/assets/pdf_file/0003/371145/who-hen-report-56.pdf?ua=1

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
57
58. Schünemann HJ, Hill SR, Kakad M, Vist GE, Bellamy R, Stockman L, et al. Transparent Development of the WHO Rapid
Advice Guidelines. PLoS Medicine. 2007;4(5):e119-e.
59. Battista RN, Hodge MJ. Setting priorities and selecting topics for clinical practice guidelines. CMAJ. 1995;153(9):1233-7.
60. Oxman AD, Schünemann HJ, Fretheim A. Improving the use of research evidence in guideline development: 2. Priorit
y
s
etting. Health Research Policy and Systems. 2006;4(1):14.
61. European Centre for Disease Prevention and Control. Infectious diseases of specific relevance to nearly-arrived migrants in
the EU/EEA. Stockholm: ECDC, 2015. Available at:
https://ecdc.europa.eu/sites/portal/files/media/en/publications/Publications/Infectious-diseases-of-specific-relevance-to-
newly-arrived-migrants-in-EU-EEA.pdf.
62. European Centre for Disease Prevention and Control. Meeting report: Evidence-based guidance for the prevention of
in
fectious diseases among newly arrived migrants to the EU/EEA. Stockholm: ECDC, 2015.
63. Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M, et al. GRADE guidelines: 8. Rating the quality o
f
e
vidence—indirectness. Journal of Clinical Epidemiology. 2011;64(12):1303-10.
64. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review
and meta-analysis protocols (PRISMA-P) 2015 statement. Systematic Reviews. 2015;4(1):1.
65. Shea BJ, Grimshaw JM, Well GA, Boers M, Andersson N, Hamel C, et al. Development of AMSTAR: a measurement tool to
assess the methodological quality of systematic reviews. BMC Med Res Methodol. 2007;7:10.
66. Peterson J, Welch V, Losos M, Tugwell P. The Newcastle-Ottawa scale (NOS) for assessing the quality of non-randomised
studies in meta-analyses. 2011. Available at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp
.
67. Alonso-Coello P, Schünemann HJ, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, et al. GRADE Evidence to Decision
(EtD) frameworks: a systematic and transparent approach to making well-informed healthcare choices. 1: Introduction. Br
Med J. 2016;353.
68. Drummond M, Methods for the economic evaluation of health care programmes: Oxford University Press; 2005. p.379.
69. Lewin S, Glenton C, Munthe-Kaas H, Carlsen B, Colvin CJ, Gulmezoglu M, et al. Using qualitative evidence in decision
making for health and social interventions: an approach to assess confidence in findings from qualitative evidence
syntheses (GRADE-CERQual). PLoS Med. 2015;12(10):e1001895.
70. McMaster University, Gradepro tool. GRADEpro GDT. 2017. Available at: https://cebgrade.mcmaster.ca/gradepro.html.
71. European Centre for Disease Prevention and Control. Guidance on tuberculosis control in vulnerable and hard-to-reach
populations. Stockholm: European Centre for Disease Prevention and Control. 2016. Available at:
https://ecdc.europa.eu/en/publications-data/public-health-guidance-tuberculosis-control-vulnerable-and-hard-reach-
populations
72. Lönnroth K, Migliori GB, Abubakar I, D'Ambrosio L, de Vries G, Diel R, et al. Towards tuberculosis elimination: an action
framework for low-incidence countries. The European Respiratory Journal. 2015;45(4):928-52.
73. European Centre for Disease Prevention and Control. Progressing towards TB elimination. Stockholm: ECDC, 2010.
A
vailable at: https://ecdc.europa.eu/en/publications-data/progressing-towards-tb-elimination.
74. European Centre for Disease Prevention and Control and World Health Organization Regional Office for Europe.
T
uberculosis surveillance and monitoring in Europe 2017. Stockholm ECDC, 2017. Available at:
https://ecdc.europa.eu/en/publications-data/tuberculosis-surveillance-and-monitoring-europe-2017.
75. Ködmön C, Zucs P, van der Werf M. Migration-related tuberculosis: epidemiology and characteristics of tuberculosis cases
originating outside the European Union and European Economic Area, 2007 to 2013. Euro Surveill. 2016;21:12.
76. European Centre for Disease Prevention and Control and World Health Organization Regional Office for Europe.
T
uberculosis surveillance and monitoring in Europe 2018 – 2016 data. Stockholm: ECDC, 2018. Available at:
https://ecdc.europa.eu/en/publications-data/tuberculosis-surveillance-and-monitoring-europe-2018.
77. Hollo V, Beauté J, Ködmön C, van der Werf MJ. Tuberculosis notification rate decreases faster in residents of native origin
than in residents of foreign origin in the EU/EEA, 2010 to 2015. Eurosurveillance. 2017;22(12):30486.
78. Hollo V, Kotila S, Kodmon C, Zucs P, Van der Werf MJ. The effect of migration within the European Union/European
Economic Area on the distribution of tuberculosis, 2007-2013. Euro Surveill. 2016;21(12):pii=30171.
79. Dara M, Solovic I, Sotgiu G, D'Ambrosio L, Centis R, Tran R, et al. Tuberculosis care among refugees arriving in Europe: An
ERS/WHO Europe Region survey of current practices. European Respiratory Journal. 2016;48(3):808-17.
80. Pareek M, Greenaway C, Noori T, Munoz J, Zenner D. The impact of migration on tuberculosis epidemiology and control in
high-income countries: a review. BMC Medicine. 2016;14(1):48.
81. Pareek M, Baussano I, Abubakar I, Dye C, Lalvani A. Evaluation of Immigrant Tuberculosis Screening in Industrialized
Countries. Emerging Infectious Diseases. 2012;18:1422-9.
82. Klinkenberg E, Manissero D, Semenza J, Verver S. Migrant tuberculosis screening in the EU/EEA: yield, coverage and
limitations. European Respiratory Journal. 2009;34(5):1180-9.
83. Arshad S, Bavan L, Gajari K, Paget SN, Baussano I. Active screening at entry for tuberculosis among new immigrants: a
systematic review and meta-analysis. European Respiratory Journal. 2010;35(6):1336-45.
84. Aldridge RW, Yates TA, Zenner D, White PJ, Abubakar I, Hayward AC. Pre-entry screening programmes for tuberculosis in migrants to
low-incidence countries: a systematic review and meta-analysis. The Lancet Infectious Diseases. 2014;14(12):1240-9.
85. Van’t Hoog A, Langendam M, Mitchell E, Cobelens F, Sinclair D, Leeflang M, et al. A systematic review of the sensitivity and
specificity of symptom-and chest-radiography screening for active pulmonary tuberculosis in HIV-negative persons and
persons with unknown HIV status. Systematic Review #2 for WHO Document- Systematic screening for active tuberculosis:
principles and recommendations.Geneva, Switzerland: WHO, 2013.
86. Pinto LM, Pai M, Dheda K, Schwartzman K, Menzies D, Steingart KR. Scoring systems using chest radiographic features for
the diagnosis of pulmonary tuberculosis in adults: a systematic review. Eur Resp J. 2013;42(2):480-94.
87. Mitchell EMH, Shapiro A, Golub J, Kranzer K, Portocarrero AV, Najlis CA, et al. Acceptability of TB Screening Among At-Ris
k
a
nd Vulnerable Groups: A Systematic Qualitative/Quantitative Literature Metasynthesis Systematic Review #4a for WHO
.
Sys
tematic screening for active tuberculosis: principles and recommendations. Geneva, Switzerland: World Heatlh
Organization, 2013.
88. World Health Organization. Systematic Screening for Active Tuberculosis: Principles & Recommendations. Geneva,
Switzerland: World Health Organization, 2013.

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
58
89. Schwartzman K, Menzies D. Tuberculosis screening of immigrants to low-prevalence countries: a cost-effectiveness
analysis. American Journal of Respiratory and Critical Care Medicine. 2000;161(3):780-9.
90. Dasgupta K, Schwartzman K, Marchand R, Tennenbaum TN, Brassard P, Menzies D. Comparison of cost-effectiveness o
f
t
uberculosis screening of close contacts and foreign-born populations. American Journal of Respiratory and Critical Care
Medicine. 2000;162(6):2079-86.
91. Oxlade O, Schwartzman K, Menzies D. Interferon-gamma release assays and TB screening in high-income countries: a cost-
effectiveness analysis. The International Journal of Tuberculosis and Lung Disease. 2007;11(1):16-26.
92. Rechel B, Mladovsky P, Ingleby D, Mackenbach JP, McKee M. Migration and health in an increasingly diverse Europe. Th
e
L
ancet. 2013;381:1235-45.
93. Seedat F, Hargreaves S, Nellums LB, Ouyang J, Brown M, Friedland JS, et al. How effective are approaches to migrant
screening for infectious diseases in Europe? A systematic review. The Lancet Infectious Diseases. 2018 Sep;18(9):e259-e271.
94. Menzies D, Benedetti A, Paydar A, Martin I, Royce S, Pai M, et al. Effect of duration and intermittency of rifampin on
tuberculosis treatment outcomes: a systematic review and meta-analysis. PLoS Med. 2009;6(9):e1000146.
95. Yee D, Valiquette C, Pelletier M, Parisien I, Rocher I, Menzies D. Incidence of serious side effects from first-line
antituberculosis drugs among patients treated for active tuberculosis. Am J Respir Crit Care Med. 2003;167(11):1472-7.
96. European Centre for Disease Prevention and Control (ECDC)/World Health Organization Regional Office for Europe.
Tuberculosis surveillance and monitoring in Europe 2017. Stockholm: ECDC, 2017.
97. Nahid P, Dorman SE, Alipanah N, Barry PM, Brozek JL, Cattamanchi A, et al. Official American Thoracic Society/Centers for
Disease Control and Prevention/Infectious Diseases Society of America Clinical Practice Guidelines: Treatment of Drug-
Susceptible Tuberculosis. Clinical Infectious Diseases. 2016;63(7):e147-e95.
98. European Centre for Disease Prevention and Control. Guidance on tuberculosis control in vulnerable and hard-to-reach
populations. Stockholm: ECDC, 2016. Available at:
https://
www.ecdc.europa.eu/sites/portal/files/media/en/publications/Publications/TB-guidance-interventions-vulnerable-
groups.pdf.
99. Liu Q, Abba K, Alejandria MM, Sinclair D, Balanag VM, Lansang MAD. Reminder systems to improve patient adherence to
t
uberculosis clinic appointments for diagnosis and treatment. The Cochrane Library. 2014. Cochrane Database Syst Re
v.
2
014 Nov 18;(11):CD006594.
100. Lutge EE, Wiysonge CS, Knight SE, Sinclair D, Volmink J. Incentives and enablers to improve adherence in tuberculosis. The
Cochrane Library. 2015. Cochrane Database Syst Rev. 2015 Sep 3;(9):CD007952.
101. Nglazi MD, Bekker L-G, Wood R, Hussey GD, Wiysonge CS. Mobile phone text messaging for promoting adherence to anti-
tuberculosis treatment: a systematic review. BMC Infectious Diseases. 2013;13(1):1.
102. European Centre for Disease Prevention and Control. HIV and migrants. Monitoring implementation of the Dublin
Declaration on Partnership to Fight HIV/AIDS in Europe and Central Asia. Stockholm: 2017. Available at:
https://ecdc.europa.eu/sites/portal/files/documents/HIV%20and%20migrants.pdf.
103. Australian Panel Member Instructions: Immigration Medical Examinations. Australian Government Department of Home
Affairs, July 2018.
104. Fakoya I, Reynolds R, Caswell G, Shiripinda I. Barriers to HIV testing for migrant black Africans in Western Europe. HIV
Medicine. 2008;9:23-5.
105. Public Health Agency of Canada. Canadian Tuberculosis Standards. Chapter 13: Tuberculosis Surveillance and Screening in
Selected High-Risk Populations. 2014. Available at: https://www.canada.ca/en/public-health/services/infectious-
diseases/canadian-tuberculosis-standards-7th-edition/edition-9.html.
106. Fakoya I, Álvarez-del Arco D, Woode-Owusu M, Monge S, Rivero-Montesdeoca Y, Delpech V, et al. A systematic review of
post-migration acquisition of HIV among migrants from countries with generalised HIV epidemics living in Europe:
implications for effectively managing HIV prevention programmes and policy. BMC Public Health. 2015;15(1):561.
107. Panel Members’ Handbook. Government of Canada, 2013. Immigration Medical Examination Instructions: Tuberculosis
.
G
overnment of Canada, November 2013.
108. Government of Canada. Operations Directorate, health Branch, Immigration Medical Examination Instructions:
Tuberculosis. 01 November 2013. Available at:
https://www.canada.ca/content/dam/ircc/migration/ircc/english/department/partner/pp/pdf/imei_tuberculosis.pdf
109. La ministre des solidarités et de la santé. Direction générale de la santé. Instruction No.
D
GS/SP1/DGOS/SDR4/DSS/SD2/DGCS/2018/143 du 8 juin 2018 relative à la mise en place du parcours de santé des
migrants primo-arrivants. [Instructions relating to the implementation of health examinations for newly-arrived migrants].
Available at: http://circulaires.legifrance.gouv.fr/pdf/2018/07/cir_43755.pdf
.
110. Public Health England. UK Visas and Immigration UK tuberculosis technical instructions (UKTBTI) Version 6. 2013
September 2013.
111. Kunst H, Burman M, Arnesen TM, Fiebig L, Hergens MP, Kalkouni O, et al. Tuberculosis and latent tuberculous infection
screening of migrants in Europe: comparative analysis of policies, surveillance systems and results. The Internationa
l
J
ournal of Tuberculosis and Lung Disease. 2017;21(8):840-51.
112. UNAIDS. 90-90-90: An ambitious treatment target to help end the AIDS epidemic. Geneva: 2014. Available at:
http://www.unaids.org/sites/default/files/media_asset/90-90-90_en.pdf
.
113. US Centers for Disease Control and Prevention. CDC Immigration Requirements: Technical Instructions for Tuberculosis
Screening and Treatment Using Cultures and Directly Observed Therapy In: Technical Instructions for Medical Examination
of Aliens. 2009.
114. van der Werf MJ, Zellweger JP. Impact of migration on tuberculosis epidemiology and control in the EU/EEA.
Eurosurveillance. 2016;21(12):30174.
115. Getahun H, Matteelli A, Abubakar I, Aziz MA, Baddeley A, Barreira D, et al. Management of latent Mycobacterium
tuberculosis infection: WHO guidelines for low tuberculosis burden countries. European Respiratory Journal.
2015;46(6):1563-76.
116. Eurostat. European social statistics 2013. Available at: https://ec.europa.eu/eurostat/web/products-pocketbooks/-/KS-FP-13-001.
117. Houben RM, Dodd PJ. The Global Burden of Latent Tuberculosis Infection: A Re-estimation Using Mathematical Modelling
.
PLoS Med. 2016;13(10):e1002152.

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
59
118. World Health Organization. Latent tuberculosis infection: updated and consolidated guidelines for programmatic
management. Geneva: World Health Organization, 2018.
119. Pai M, Zwerling A, Menzies D. Systematic review: T-cell–based assays for the diagnosis of latent tuberculosis infection: an
update. Ann Intern Med. 2008;149(3):177-84.
120. Kik SM RM. Predictive utility of the tuberculin skin test and interferon-gamma release assay among individuals who are
not
prescribed tuberculosis preventive therapy. Systematic Review # 4 for WHO Document "Guidelines on the management of
la
tent tuberculosis infection". Geneva, Switzerland: World Health Organization, 2014.
121. Kahwati LC, Feltner C, Halpern M, Woodell CL, Boland E, Amick HR, et al. Primary care screening and treatment for latent
tuberculosis infection in adults: evidence report and systematic review for the US Preventive Services Task Force. JAMA.
2016;316(9):970-83.
122. Stagg HR, Zenner D, Harris RJ, Munoz L, Lipman MC, Abubakar I. Treatment of latent tuberculosis infection: a network
met
a-analysis. Ann Inter Med. 2014;161(6):419-28.
123. Sharma SK, Sharma A, Kadhiravan T, Tharyan P. Rifamycins (rifampicin, rifabutin and rifapentine) compared to isoniazid for
preventing tuberculosis in HIV-negative people at risk of active TB. Evidence-Based Child Health: A Cochrane Review
Journal. 2014;9(1):169-294.
124. Alsdurf H, Hill PC, Matteelli A, Getahun H, Menzies D. The cascade of care in diagnosis and treatment of latent tuberculosis
infection: a systematic review and meta-analysis. The Lancet Infectious Diseases. 2016;16(11):1269-78.
125. Sandgren A, Noordegraaf-Schouten MV, van Kessel F, Stuurman A, Oordt-Speets A, van der Werf MJ. Initiation and
completion rates for latent tuberculosis infection treatment: a systematic review. BMC Infectious Diseases. 2016;16(1):1.
126. Pareek M, Watson JP, Ormerod LP, Kon OM, Woltmann G, White PJ, et al. Screening of immigrants in the UK for imported
latent tuberculosis: a multicentre cohort study and cost-effectiveness analysis. The Lancet Infectious Diseases.
2
011;11(6):435-44.
127. Pareek M, Bond M, Shorey J, Seneviratne S, Guy M, White P, et al. Community-based evaluation of immigrant tuberculosis
screening using interferon-release assays and tuberculin skin testing: observational study and economic analysis.. Thorax
.
2
013 Mar;68(3):230-9.
128. Hardy AB, Varma R, Collyns T, Moffitt SJ, Mullarkey C, Watson JP. Cost-effectiveness of the NICE guidelines for screening
for latent tuberculosis infection: the QuantiFERON-TB Gold IGRA alone is more cost-effective for immigrants from high
burden countries. Thorax. 2010;65(2):178-80.
129. Iqbal AZ, Leighton J, Anthony J, Knaup RC, Peters EB, Bailey TC. Cost-effectiveness of Using Quantiferon Gold (QFT-G)®
versus Tuberculin Skin Test (TST) among US and Foreign Born Populations at a Public Health Department Clinic with a Low
Prevalence of Tuberculosis. Public Health Nursing. 2014;31(2):144-52.
130. Linas BP, Wong AY, Freedberg KA, Horsburgh Jr CR. Priorities for screening and treatment of latent tuberculosis infection in
the United States. Am J Respir Crit Care Med. 2011;184(5):590-601.
131. Deuffic-Burban S, Atsou K, Viget N, Melliez H, Bouvet E, Yazdanpanah Y. Cost-effectiveness of QuantiFERON®-TB test vs.
tuberculin skin test in the diagnosis of latent tuberculosis infection. The International Journal of Tuberculosis and Lung
Disease. 2010;14(4):471-81.
132. Pooran A, Booth H, Miller RF, Scott G, Badri M, Huggett JF, et al. Different screening strategies (single or dual) for the
diagnosis of suspected latent tuberculosis: a cost effectiveness analysis. BMC Pulmonary Medicine. 2010;10(1):1.
133. Greenaway C, Sandoe A, Vissandjee B, Kitai I, Gruner D, Wobeser W, et al. Tuberculosis: evidence review for newly
arriving immigrants and refugees. Canadian Medical Association Journal. 2011;183(12):E939-E51.
134. Munro SA, Lewin SA, Smith HJ, Engel ME, Fretheim A, Volmink J. Patient adherence to tuberculosis treatment: a systematic
review of qualitative research. PLoS Med. 2007;4(7):e238.
135. Tomás BA, Pell C, Cavanillas AB, Solvas JG, Pool R, Roura M. Tuberculosis in migrant populations. A systematic review o
f
t
he qualitative literature. PLOS one. 2013;8(12):e82440.
136. Stuurman AL, Noordegraaf-Schouten MV, van Kessel F, Oordt-Speets AM, Sandgren A, van der Werf MJ. Interventions for
improving adherence to treatment for latent tuberculosis infection: a systematic review. BMC Infectious Diseases. 2016;16(1):1.
137. M'Imunya JM, Kredo T, Volmink J. Patient education and counselling for promoting adherence to treatment for tuberculosis
.
T
he Cochrane Library. 2012(5). Available at: https://
www.cap-
tb.org/sites/default/files/documents/Cochrane.PatientAdherence.Counselling.TB.pdf.
138. Griffiths C, Sturdy P, Brewin P, Bothamley G, Eldridge S, Martineau A, et al. Educational outreach to promote screening for
tuberculosis in primary care: a cluster randomised controlled trial. The Lancet. 2007;369(9572):1528-34.
139. D’Ambrosio L, Centis R, Dara M, Solovic I, Sulis G, Zumla A, et al. European policies in the management of tuberculosis
among migrants. Inter J Infect Dis. 2017.56, 85–89.
140. La ministre des solidarités et de la santé. Recommandations relatives à la lutte antituberculeuse chez les migrants en
France, 2005. [Recommendations to prevent tuberculosis among migrants in France.] Available at: https://solidarites-
sante.gouv.fr/IMG/pdf/Avis_30_septembre_2005_relatif_aux_recommandations_relatives_a_la_lutte_antituberculeuse_chez
_les_migrants_en_France.pdf.
141. Public Health England. Guidance: Tuberculosis Screening, Latent TB infection (LTBI) 2014 [10 April 2018]. Available at:
https://www.gov.uk/guidance/tuberculosis-screening#latent-tb-infection-ltbi
.
142. US Centers for Disease Control and Prevention. Refugee Health Guidelines. Immigrant and Refugee Health. CDC. 2013.
Available at: https://www.cdc.gov/immigrantrefugeehealth/guidelines/refugee-guidelines.html
.
143. US Centers for Disease Control and Prevention. Chapter-8 Newly Arrived Immigrants & Refugees. CDC 2017. Available at:
https://wwwnc.cdc.gov/travel/yellowbook/2018/advising-travelers-with-specific-needs/newly-arrived-immigrants-refugees.
144. Lewinsohn DM, Leonard MK, LoBue PA, Cohn DL, Daley CL, Desmond E, et al. Official American Thoracic Society/Infectious
Diseases Society of America/US Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosis o
f
T
uberculosis in Adults and Children. Clin Infect Dis. 2017;64(2):e1-e33.
145. European Centre for Disease Prevention and Control/WHO Regional Office for Europe. HIV/AIDS surveillance in Europe
2017 – 2016 data. Stockholm: ECDC, 2017. Available at: https://ecdc.europa.eu/en/publications-data/hivaids-surveillance-
europe-2017-2016-data
146. Pharris A, Quinten C, Noori T, Amato-Gauci AJ, van Sighem A. Estimating HIV incidence and number of undiagnosed
individuals living with HIV in the European Union/European Economic Area, 2015. Eurosurveillance. 2016;21(48):30417.

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
60
147. World Health Organization. HIV assays: laboratory performance and other operational characteristics: rapid diagnostic tests
(combined detection of HIV-1/2 antibodies and discriminatory detection of HIV-1 and HIV-2 antibodies): Report 18.
Geneva: WHO, 2015.
148. Alvarez-del Arco D, Monge S, Azcoaga A, Rio I, Hernando V, Gonzalez C, et al. HIV testing and counselling for migrant
populations living in high-income countries: a systematic review. European Journal of Public Health. 2013;23:1039-45.
149. Salama P, Dondero, TJ. HIV surveillance in complex emergencies. AIDS. 2001;15(Supplement 3):S4-S12.
150. Pottie K, Medu O, Welch V, Dahal GP, Tyndall M, Rader T, et al. Effect of rapid HIV testing on HIV incidence and services in
populations at high risk for HIV exposure: an equity-focused systematic review. BMJ Open. 2014;4(12).
151. Rice BD, Elford J, Delpech VC. A new method to assign country of HIV infection among heterosexuals born abroad and
diagnosed with HIV. AIDS. 2012;26(15):1961-6.
152. Alvarez-del Arco D, Fakoya I, Thomadakis C, Pantazis N, Touloumi G, Gennotte A-F, et al. High levels of postmigration HIV
acquisition within nine European countries. AIDS. 2017;31(14):1979-88.
153. Pottie K, Vissandjée B, Grant J. Human immunodeficiency virus. Evidence review for newly arriving immigrants and
refugees: Appendix to Pottie K, Greenaway C, Feightner J, et al. Evidence-based clinical guidelines for immigrants and
refugees. CMAJ 2011 Sep 6; 183(12): E824–E925.
154. World Health Organization. Consolidated guidelines on HIV testing services. Geneva: WHO, 2015.
155. European Centre for Disease Prevention and Control. HIV Testing: increasing uptake and effectiveness in the European
Union. Stockholm: ECDC, 2010. Available at:
https://ecdc.europa.eu/sites/portal/files/media/en/publications/Publications/101129_GUI_HIV_testing.pdf
156. Mounier-Jack S, Nielsen S, Coker RJ. HIV testing strategies across European countries. HIV Medicine. 2008;9(2):13-9.
157. Alvarez-Del Arco D, Monge S, Caro-Murillo AM, Ramirez-Rubio O, Azcoaga-Lorenzo A, Belza MJ, et al. HIV testing policies
for migrants and ethnic minorities in EU/EFTA Member States. European Journal of Public Health. 2014;24:139-44.
158. Kennedy CE, Fonner VA, Sweat MD, Okero FA, Baggaley R, O’Reilly KR. Provider-Initiated HIV Testing and Counseling in
Low- and Middle-Income Countries: A Systematic Review. AIDS and Behavior. 2013;17(5):1571-90.
159. Desai M, Woodhall SC, Nardone A, Burns F, Mercey D, Gilson R. Active recall to increase HIV and STI testing: a systematic
review. Sexually Transmitted Infections. 2015;91(5):314-23.
160. Chou R, Selph S, Dana T, et al. Screening for HIV: Systematic review to update the 2005 U.S. Preventive Services Tas
k
F
orce Recommendation. Annals of Internal Medicine. 2012;157(10):706-18.
161. Walensky RP, Morris BL, Reichmann WM, Paltiel AD, Arbelaez C, Donnell-Fink AL, et al. Counselor-Versus Provider-Based
HIV Screening in the Emergency Department: Results From the Universal Screening for HIV Infection in the Emergency
Room (USHER) Randomized Controlled Trial. . Annals of Emergency Medicine. 2011;58(Supplement 1):s126-S32.
162. Cohen MS, Chen YQ, McCauley M, Gamble T, Hosseinipour MC, Kumarasamy N, et al. Prevention of HIV-1 Infection with
Early Antiretroviral Therapy. New England Journal of Medicine. 2011;365(6):493-505.
163. Lundgren JD, Babiker AG, Gordin F, Emery S, Grund B, Sharma S, et al. Initiation of Antiretroviral Therapy in Early
Asymptomatic HIV Infection. New England Journal of Medicine. 2015;373(9):795-807.
164. World Health Organization. Guidelines on when to start antiretroviral therapy and on pre-exposure prophylaxis for HIV
.
G
eneva, Switzerland: WHO; 2015.
165. Muessig KE, Smith MK, Powers KA, Lo Y-R, Burns DN, Grulich AE, et al. Does ART prevent HIV transmission among MSM?
AIDS (London, England). 2012;26(18):2267-73.
166. Farnham PG, Gorsky RD, Holtgrave DR, Jones WK, Guinan ME. Counseling and testing for HIV prevention: costs, effects,
a
nd cost-effectiveness of more rapid screening tests. Public Health Reports. 1996;111(1):44-54.
167. Kassler WJ, Dillon BA, Haley C, Jones WK, Goldman A. On-site, rapid HIV testing with same-day results and counseling
.
A
IDS. 1997;11(8):1045-51.
168. Wilkinson D, Wilkinson N, Lombard C, Martin D, Smith A, Floyd K, et al. On-site HIV testing in resource-poor settings: is
one rapid test enough? AIDS. 1997;11(3):377-81.
169. Kallenborn JC, Price TG, Carrico R, Davidson AB. Emergency Department Management of Occupational Exposures: Cost
Analysis of Rapid HIV Test. Infection Control and Hospital Epidemiology. 2001;22(5):289-93.
170. Ekwueme DU, Pinkerton SD, Holtgrave DR, Branson BM. Cost comparison of three HIV counseling and testing technologies
.
A
merican Journal of Preventive Medicine. 2003;25(2):112-21.
171. Doyle NM, Levison JE, Gardner MO. Rapid HIV versus enzyme-linked immunosorbent assay screening in a low-risk Mexican American
population presenting in labor: A cost-effectiveness analysis. American Journal of Obstetrics and Gynecology. 2005;193(3):1280-5.
172. Paltiel AD, Weinstein MC, Kimmel AD, Seage GR, Losina E, Zhang H, et al. Expanded Screening for HIV in the United States
— An Analysis of Cost-Effectiveness. New England Journal of Medicine. 2005;352(6):586-95.
173. Vickerman P, Terris-Prestholt F, Delany S, Kumaranayake L, Rees H, Watts C. . Are targeted HIV prevention activities cost-
effective in high prevalence settings? Results from a sexually transmitted infection treatment project for sex workers in
Johannesburg, South Africa. Sexually transmitted diseases. Transmitted Diseases. 2006;33(10):S122-S32.
174. Marks G, Crepaz N, Janssen RS. Estimating sexual transmission of HIV from persons aware and unaware that they are
infected with the virus in the USA. AIDS. 2006;20:1447-50.
175. Hernando V, Alvárez-del Arco D, Alejos B, Monge S, Amato-Gauci AJ, Noori T, et al. HIV Infection in Migrant Populations in
the European Union and European Economic Area in 2007–2012: An Epidemic on the Move. Journal of Acquired Immune
Deficiency Syndromes. 2015;70(2).
176. European Centre for Disease Prevention and Control. Evidence brief: Impact of stigma and discrimination on access to HIV
services in Europe. Monitoring implementation of the Dublin Declaration on partnership to fight HIV/AIDS in Europe and
Central Asia. Stockholm: ECDC; 2017. Available at: https://ecdc.europa.eu/sites/portal/files/documents/Dublin-EB-
Stigma%20and%20discrimination%202017_final.pdf
177. Blondell SJ, Kitter B, Griffin MP, Durham J. Barriers and Facilitators to HIV Testing in Migrants in High-Income Countries: A
Systematic Review. AIDS and Behavior. 2015;19(11):2012-24.
178. Deblonde J, De Koker P, Hamers FF, Fontaine J, Luchters S, Temmerman M. Barriers to HIV testing in Europe: a systematic
review. European Journal of Public Health. 2010;20(4):422-32.
179. Arco DAD, Monge S, Caro-Murillo AM, Ramïrez-Rubio O, Azcoaga-Lorenzo A, Belza MJ, et al. HIV testing policies for
migrants and ethnic minorities in EU/EFTA Member States. European Journal of Public Health. 2014;24(1):139-44.

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
61
180. European Centre for Disease Prevention and Control. Antenatal screening for HIV, hepatitis B, syphilis and rubella susceptability in the
EU/EEA. Stockholm: ECDC, 2017. Available at: https://ecdc.europa.eu/sites/portal/files/media/en/publications/Publications/antenatal-
screening-HIV-hepatitis-B-syphilis-rubella-EU.pdf
181. European AIDS Clinical Society. European guidelines for the treatment of HIV-positive adults in Europe. Version 9.1,
October 2018. Available at: http://www.eacsociety.org/files/2018_guidelines-9.1-english.pdf
182. Rice BD, Elford J, Yin Z, Delpech VC. A new method to assign country of HIV infection among heterosexuals born abroad
and diagnosed with HIV. AIDS. 2012;26(15):1961-6.
183. Desgrees-du-Lou A, Pannetier J, Ravalihasy A, Gosselin A, Supervie V, Panjo H, et al. Sub-Saharan African migrants living
with HIV acquired after migration, France, ANRS PARCOURS study, 2012 to 2013. Euro Surveill. 2015;20(46).
184. Desgrees-du-Lou A, Pannetier J, Ravalihasy A, Le Guen M, Gosselin A, Panjo H, et al. Is hardship during migration a
determinant of HIV infection? Results from the ANRS PARCOURS study of sub-Saharan African migrants in France. AIDS.
2016;30(4):645-56.
185. Réévaluation de la stratégie de dépistage de l’infection à VIH en France. . Haute Autorité de Santé; 2017 March 2017.
186. HIV: Migrant Health Guide: Public Health England; London: PHE, 2014 [updated 31 July 2014 and 18 July 2018]. Available
from: https://www.gov.uk/guidance/hiv-migrant-health-guide
.
187. HIV Testing in England: 2017 report. Public Health England; London: PHE 2017. Available at:
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/666478/HIV_testing_in
_England_2017_report.pdf.
188. World Health Organization. Global hepatitis report. Geneva: WHO, 2017.
189. Pitigoi D, Rafila A, Pistol A, Arama V, Molagic V, Streinu-Cercel A. Trends in hepatitis B incidence in Romania, 1989-2005.
Eurosurveillance. 2008;13(2):11-2%P 8012.
190. World Health Organization. Guidelines on Hepatitis B and C testing. Geneva: WHO, 2017.
191. Rossi C, Shrier I, Marshall L, Cnossen S, Schwartzman K, Klein MB, et al. Seroprevalence of Chronic Hepatitis B Virus
Infection and Prior Immunity in Immigrants and Refugees: A Systematic Review and Meta-Analysis. PLoS ONE.
2012;7(9):e44611-e.
192. Rossi C, Schwartzman K, Oxlade O, Klein MB, Greenaway C, et al. Hepatitis and Vaccination Strategies for Newly Arrived
Adult Canadian Immigrants and Refugees: Analysis. PLoS One 2013 Oct 18;8(10).
193. European Centre for Disease Prevention and Control. Hepatitis B and C testing activities, needs, and priorities in the
EU/EEA. Stockholm: ECDC, 2017. Available at: https://ecdc.europa.eu/en/publications-data/hepatitis-b-and-c-testing-
activities-needs-and-priorities-eueea.
194. European Centre for Disease Prevention and Control. Antenatal screening approaches effective in preventing mother-child-
transmission of HIV, hepatitis B, syphilis and rubella in vulnerable populations. Stockholm: ECDC; 2017
.
h
ttps://ecdc.europa.eu/sites/portal/files/media/en/publications/Publications/antenatal-screening-approaches-to-prevent-
MTCT-of-HIV-HBV-syphilis-rubella-lit-review-2017.pdf
195. Schweitzer A, Horn J, Mikolajczyk RT, Krause G, Ott JJ, et al. Estimations of worldwide prevalence of chronic hepatitis C virus infection:
a systematic review of data published between 1965 and 2013. The Lancet Infectious Diseases. 2015;386 (10003):1546-55.
196. Chou R, Dana T, Bougatsos C, Blazina I, Zakher B, Khangura J. Screening for Hepatitis B Virus Infection in Nonpregnant
Adolescents and Adults: Systematic Review to Update the 2004 U.S. Preventive Services Task Force Recommendation.
Rockville (MD): Agency for Healthcare Research and Quality, 2014.
197. Wong GLH, Yiu KKL, Wong VWS, Tsoi KKF, Chan HLY. Meta-analysis: Reduction in hepatic events following interferon-alfa
therapy of chronic hepatitis B. Aliment Pharmacol Ther. 2010;32(9):1059-68.
198. Graham S, Guy RJ, Cowie B, Wand HC, Donovan B, Akre SP, et al. Chronic hepatitis B prevalence among Aboriginal and
Torres Strait Islander Australians since universal vaccination: a systematic review and meta-analysis 2013. BMC Infect Dis
.
2
013 08 31;13(1):403.
199. European Centre for Disease Prevention and Control. Epidemiological assessment of hepatitis B and C among migrants in
the EU/EEA. Stockholm: ECDC; 2016.
https://ecdc.europa.eu/sites/portal/files/media/en/publications/Publications/epidemiological-assessment-hepatitis-B-and-C-
among-migrants-EU-EEA.pdf
200. European Association for the Study of the Liver. EASL Recommendations on Treatment of Hepatitis C - 2016. Journal of
H
epatology. 2017;66(1):153-94.
201. World Health Organization. Guidelines for the prevention, care and treatment of persons with chronic hepatitis B infection. Geneva:
WHO, 2015.
202. Chang MH, You SL, Chen CJ, Liu CJ, Lee CM, Lin SM, et al. Decreased incidence of hepatocellular carcinoma in hepatitis
B
vaccinees: A 20-year follow-up study. Cancer Inst. 2009;101:1348-55.
203. Blachier M, Leleu H, Peck-Radosavljevic M, Valla D, Roudot-Thoraval F, J. C, The burden of liver disease in Europe: A
review of available epidemiological data 2009. J Hepatol. 2013 Mar; 58(3):593-608.
204. Duffell E, Hedrich D, Mardh O, Mozalevskis A. Towards Elimination of hepatitis B and C in European Union and European
Economic Area Countries: Monitiroing World Health Organization's global health sector strategy core indicators and scaling
up key interventions. Euro Surveill 2017;22(9):pii=30476.
205. LeFevre ML. Screening for hepatitis B virus infection in nonpregnant adolescents and adults: U.S. preventive services task
force recommendation statement. Vol Annals of Internal Medicine 2014;161:58-66.
206. Rossi C, Schwartzman K, Oxlade O, Klein MB, Greenaway C. Hepatitis B Screening and Vaccination Strategies for Newly
Arrived Adult Canadian Immigrants and Refugees: A Cost-Effectiveness Analysis. PLOS ONE. 2013;8(10):e78548.
207. Wong WWL, Woo G, Heathcote E, Krahn M. Cost effectiveness of screening immigrants for hepatitis B. Liver Int. 2011;31(8):1179-90.
208. Hutton DW, Tan D, So SK, Brandeau ML. Cost-effectiveness of screening and vaccinating Asian and Pacific Islander adults
for hepatitis B. Ann Intern Med. 2007;147(7):460-9.
209. Veldhuijzen IK, Toy M, Hahne SJ, De Wit GA, Schalm SW, de Man RA, et al. Screening and Early Treatment of Migrants for
Chronic Hepatitis B Virus Infection Is Cost-Effective. Gastroenterology. 2010;138(2):522-30.
210. Rein DB, Lesesne SB, Smith BD, Weinbaum CM. Models of community-based hepatitis B surface antigen screening
programs in the U.S. and their estimated outcomes and costs. Public health reports (Washington, DC: 1974).
2011;126(4):560-7.

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
62
211. Jazwa A, Coleman MS, Gazmararian J, Wingate LMT, Maskery B, Mitchell T, et al. Cost-benefit comparison of two proposed
overseas programs for reducing chronic Hepatitis B infection among refugees: is screening essential? Vaccine.
2015;33(11):1393-9.
212. Ruggeri M, Cicchetti A, Gasbarrini A. The cost-effectiveness of alternative strategies against HBV in Italy. Health policy
(Amsterdam, Netherlands). 2011;102(1):72-80.
213. Eckman MH, Kaiser TE, Sherman KE. The cost-effectiveness of screening for chronic hepatitis B infection in the United
States. Clin Infect Dis. 2011;52(11):1294-306.
214. Li S Onder FO, Xie Q, Liu Y, Toy M. Cost-effectiveness of Early Detection of Inactive and Treatment of Active Cases in a
High Endemic Chronic Hepatitis B Region. J Antivir Antiretrovir. 2013;5:154-9.
215. Hargreaves S, Seedat F, Car J, Escombe R, Hasan S, Eliahoo J, et al. Screening for latent TB, HIV, and hepatitis B/C in new
migrants in a high prevalence area of London, UK: a cross-sectional study. BMC Infect Dis, 2014:14,657.
216. Do TN, Nam S. Knowledge, Awareness and Medical Practice of Asian Americans/Pacific Islanders on Chronic Hepatitis B
Infection: Review of Current Psychosocial Evidence. Pogon sahoe yon'gu. 2011;31(3):341.
217. Owiti JA, Greenhalgh T, Sweeney L, Foster GR, Bhui KS. Illness perceptions and explanatory models of viral hepatitis B & C
among immigrants and refugees: a narrative systematic review. BMC Public Health. 2015;15(1):151.
218. Lee A, Vedio A, Lio EZH, Horsley J, Jesurasa A, Salway S, et al. Determinants of uptake of heptitis B testing and healthcare
access by migrant Chinese in England: a qualitative study. BMC Public Health. 2017;17:747.
219. Robotin MC, George J. Community-based hepatitis B screening: what works? Hepatology International. 2014;8:478-92.
220. Herman A, Bullen C, Finau S, Ofanoa M. Mobilising Pacific people for health: insights from a hepatitis B screening
programme in Auckland, New Zealand. Pacific health dialog. 2006;13(2):9-15.
221. van der Veen YJ, van Empelen P, de Zwart O, Visser H, Mackenbach JP, Richardus JH. Cultural tailoring to promote
hepatitis B screening in Turkish Dutch: a randomized control study. Health promotion international. 2014;29(4):692-704.
222. World Health Organization. Enter the Hepatitis Testing Innovation Contest: WHO; Geneva 2016 [cited 12 June 2017].
Available from: http://www.who.int/hepatitis/news-events/hepatitis-innovation-contest/en
223. Gish RG, Cooper SL. Hepatitis B in the Greater San Francisco Bay Area: An Integrated Programme to Respond to a Diverse
Local Epidemic. Journal of Viral Hepatitis. 2011;18(4):e40-51.
224. Richter C, Beest GT, Sancak I, Aydinly R, Bulbul K, Laetemia-Tomata F, et al. Hepatitis B prevalence in the Turkish
population of Arnhem: implications for national screening policy? Epidemiology and Infection. 2012;140(4):724-30.
225. Veldhuijzen IK, Wolter R, Rijckborst V, Mostert M, Voeten HA, Cheung Y, et al. Identification and treatment of chronic
hepatitis B in Chinese migrants: Results of a project offering on-site testing in Rotterdam, the Netherlands. [cited 12 June
2018]. Journal of Hepatology. 2012;57(6):1171-6. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22885717
226. El-Hamad I, Pezzoli MC, Chiari E, Scarcella C, Vassallo F, Puoti M, et al. Point-of-care screening, prevalence, and risk factors for
hepatitis B infection among 3,728 mainly undocumented migrants from Non-EU countries in northern Italy. Med. 2015;22(2):78-86.
227. Chang MH, Chen CJ, Lai MS, Hsu HM, Wu TC, Kong MS, et al. Universal hepatitis B vaccination in Taiwan and the incidence
of hepatocellular carcinoma in children. Taiwan Childhood Hepatoma Study Group. 1997;336:1855-9.
228. Ni YH, Chang MH, Huang LM, Chen HL, Hsu HY, Chiu TY, et al. Virus infection in children and adolescents in a
hyperendemic area: 15 years after mass hepatitis B vaccination. Ann Intern Med. 2001;135(9):796-800.
229. Jefferson T, Demicheli V, Deeks J, MacMillan A, Sassi F, Pratt M. Vaccines for preventing hepatitis B in health-care workers.
Nurs Times. 2001 Nov 15-21;97(46):39.
230. Dhumeaux Daniel DJ-F, Yeni Patrick. Prise en charge thérapeutique et suivi de l’ensemble des personnes infectées par le
virus de l’hépatite C - Rapport de recommandations 2016. Conseil national du sida; Agence nationale de recherche sur le
SIDA et les hepatites virales (France); 2018 October 2016.
231. Hepatitis B: migrant health guide: Public Health England. London: PHE, 2014 [updated 28 June 2017]. Available from:
https://www.gov.uk/guidance/hepatitis-b-migrant-health-guide
.
232. Public Health England. Health protocol: pre-entry health assessments for UK-bound refugees. UK Visas and Immigration, August 2017.
Available at:
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/638386/protocolguidance.pdf
233. Public Health England. Vaccination of individuals with uncertain or incomplete immunisation status. London: PHE, 2017.
234. Mühlberger N, Schwarzer R, Lettmeier B, Sroczynski G, Zeuzem S, Siebert U. HCV-related burden of disease in Europe: a
systematic assessment of incidence, prevalence, morbidity, and mortality. BMC Public Health. 2009;9(34).
235. Mathurin P. HCV burden in Europe and the possible impact of current treatment. Dig Liver Dis. 2013;45 Suppl 5:S314-7.
236. El Khoury AC, Wallace C, Klimack WK, Razavi H. Economic burden of hepatitis C-associated diseases: Europe, Asia Pacific,
and the Americas. J Med Econ. 2012;15(5):887-96.
237. Razavi H, Robbins S, Zeuzem S, Negro F, Buti M, Duberg A-S, et al. Hepatitis C virus prevalence and level of intervention
required to achieve the WHO targets for elimination in the European Union by 2030: a modelling study. The Lancet
Gastroenterology & Hepatology. 2017;2(5):325-36.
238. Falade-Nwulia O, Suarez-Cuervo C, Nelson DR, Fried MW, Segal JB, Sulkowski MS. Oral direct-acting agent therapy for
hepatitis c virus infection: A systematic review. Annals of Internal Medicine. 2017.
239. European Centre for Disease Prevention and Control. Systematic review on hepatitis B and C prevalence in the EU/EEA.
Stockholm: ECDC, 2016. Available at:
https://ecdc.europa.eu/sites/portal/files/media/en/publications/Publications/systematic-review-hepatitis-B-C-prevalence.pdf
240. Hofstraat S, Falla A, Duffell E, Hahne S, Amato-Gauci A, Veldhuijzen I, et al. Current prevalence of chronic hepatitis B and C
virus infection in the general population, blood donors and pregnant women in the EU/EEA: a systematic review.
Epidemiology & Infection. 2017;145(14):2873-85.
241. World Health Organization Regional Office for Europe. Action plan for the health sector response to viral hepatitis in the
WHO European Region. Copenhagen: WHO/Europe, 2016.
242. International Organization for Migration. Europe/Mediterranean - Mixed Flows in the Mediterranean and Beyond - Flows
Compilation Overview 2015. OiM 2016. Available at: https://
www.iom.int/sites/default/files/situation_reports/file/Mixed-
Flows-Mediterranean-and-Beyond-Compilation-Overview-2015.pdf.
243. International Organization for Migration. Migration flows- Europe. 2016. Available at:
http://migration.iom.int/europe?type=arrivals
.

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
63
244. Eurostat. Migration and Migrant Population Statistics. 2017. Available at: https://ec.europa.eu/eurostat/statistics-
explained/index.php/Migration_and_migrant_population_statistics.
245. Falla A, Ahmad A, Duffell E, Noori T, Veldhuijzen I. Estimating the scale of chronic hepatitis C virus infection in the EU/EEA:
a focus on migrants from anti-HCV endemic countries. BMC Infect Dis 2018;18(42).
246. Greenaway C, Ma AT, Kloda LA; Klein M; Cnossen S; Schwarzer G. The Seroprevalence of Hepatitis C Antibodies in
Immigrants and Refugees from Intermediate and High Endemic Countries: A Systematic Review and Meta-Analysis. PLoS
ONE. 2015;10:e0141715.
247. Sharma S, Carballo M, Feld JJ, Janssen HL. Immigration and viral hepatitis. Journal of Hepatology. 2015;63(2):515-22.
248. Chen W, Tomlinson G, Krahn M, Heathcote J. Immigrant patients with chronic hepatitis C and advanced fibrosis have a
higher risk of hepatocellular carcinoma. Journal of Viral Hepatitis. 2012;19(8):574-80.
249. Greenaway C, Azoulay L, Allard R, Cox J, Tran VA, Chakra CNA, et al. A population-based study of chronic hepatitis C in
immigrants and non-immigrants in Quebec, Canada. BMC Infectious Diseases. 2017;17(1):140.
250. Nguyen L, Nguyen M. Systematic review: Asian patients with chronic hepatitis C infection. Alimentary Pharmacology &
Therapeutics. 2013;37(10):921-36.
251. Tiittala P, Ristola M, Liitsola K, Ollgren J, Koponen P, Surcel H-M, et al. Missed hepatitis b/c or syphilis diagnosis among
Kurdish, Russian, and Somali origin migrants in Finland: linking a population-based survey to the national infectious disease
register. BMC Infectious Diseases. 2018;18(1):137.
252. Khuroo MS, Khuroo NS, Khuroo MS. Diagnostic accuracy of point-of-care tests for hepatitis C virus infection: a systematic
review and meta-analysis. PLoS ONE. 2015;10:e0121450.
253. Kimer N, Dahl EK, Gluud LL, Krag A. Antiviral therapy for prevention of hepatocellular carcinoma in chronic hepatitis C:
systematic review and meta-analysis of randomised controlled trials. BMJ Open. 2012;2.
254. Simmons B, Saleem J, Heath K, Cooke GS, Hill A. Long-Term Treatment Outcomes of Patients Infected With Hepatitis C
Virus: A Systematic Review and Meta-analysis of the Survival Benefit of Achieving a Sustained Virological Response. Clin
Infect Dis. 2015;61(5):730-40.
255. Public Health Agency of Canada. Treatment for Hepatitis C Virus: a Systematic Review and Meta-Analysis. Ottawa:
Canadian Preventative Task Force, 2016.
256. Yehia BR, Schranz AJ, Umscheid CA, Lo Re V, 3rd. The treatment cascade for chronic hepatitis C virus infection in the
United States: a systematic review and meta-analysis. PLoS ONE. 2014;9(7):e101554.
257. Selvapatt N, Ward T, Bailey H, Bennett H, Thorne C, See L-M, et al. Is antenatal screening for hepatitis C virus cost-
effective? A decade’s experience at a London centre. Journal of Hepatology. 2015;63(4):797-804.
258. Wong WW, Erman A, Feld JJ, Krahn M. Model-based projection of health and economic effects of screening for hepatitis C
in Canada. CMAJ Open. 2017;5(3):E662.
259. Deuffic-Burban S, Obach D, Canva V, Pol S, Roudot-Thoraval F, Dhumeaux D, et al. Cost-effectiveness and budget impact
of interferon-free direct-acting antiviral-based regimens for hepatitis C treatment: the French case. Journal of Viral
Hepatitis. 2016;23(10):767-79.
260. Chhatwal J, Kanwal F, Roberts MS, Dunn MA. Cost-effectiveness and budget impact of hepatitis C virus treatment with
sofosbuvir and ledipasvir in the United States. Annals of Internal Medicine. 2015;162(6):397-406.
261. Hagan LM, Sulkowski MS, Schinazi RF. Cost analysis of sofosbuvir/ribavirin versus sofosbuvir/simeprevir for genotype 1
hepatitis C virus in interferon-ineligible/intolerant individuals. Hepatology. 2014;60(1):37-45.
262. Najafzadeh M, Andersson K, Shrank WH, Krumme AA, Matlin OS, Brennan T, et al. Cost-effectiveness of novel regimens for
the treatment of hepatitis C virus. Annals of Internal Medicine. 2015;162(6):407-19.
263. Rein DB, Wittenborn JS, Smith BD, Liffmann DK, Ward JW. The cost-effectiveness, health benefits, and financial costs of
new antiviral treatments for hepatitis C virus. Clinical Infectious Diseases. 2015;61(2):157-68.
264. Saab S, Gordon S, Park H, Sulkowski M, Ahmed A, Younossi Z. Cost-effectiveness analysis of sofosbuvir plus
peginterferon/ribavirin in the treatment of chronic hepatitis C virus genotype 1 infection. Alimentary Pharmacology &
Therapeutics. 2014;40(6):657-75.
265. Younossi Z, Park H, Saab S, Ahmed A, Dieterich D, Gordon S. Cost-effectiveness of all-oral ledipasvir/sofosbuvir regimens in
patients with chronic hepatitis C virus genotype 1 infection. Alimentary Pharmacology & Therapeutics. 2015;41(6):544-63.
266. Iyengar S, Tay-Teo K, Vogler S, Beyer P, Wiktor S, de Joncheere K, et al. Prices, costs, and affordability of new medicines
for hepatitis C in 30 countries: an economic analysis. PLoS Medicine. 2016;13(5):e1002032.
267. Marshall AD, Cunningham EB, Nielsen S, Aghemo A, Alho H, Backmund M, et al. Restrictions for reimbursement of interferon-free
direct-acting antiviral drugs for HCV infection in Europe. The Lancet Gastroenterology & Hepatology. 2018;3(2):125-33.
268. Marshall AD, Pawlotsky J-M, Lazarus JV, Aghemo A, Dore GJ, Grebely J. The removal of DAA restrictions in Europe–one
step closer to eliminating HCV as a major public health threat. Journal of Hepatology. 2018.
269. In: Institute of Medicine (US) Committee on the Prevention and Control of Viral Hepatitis Infection; Colvin HM, Mitchell AE,
editors. Washington (DC): National Academies Press (US); 2010.
270. Ferrante JM, Winston DG, Chen P-H, de la Torre AN. Family physicians' knowledge and screening of chronic hepatitis and
liver cancer. Family Medicine. 2008;40(5):345-51.
271. Fernandez M, Manzanares S, Jacques C, Caylá J, Kunkel J, Foster G. Screening for chronic viral hepatitis in migrant
populations -- Report on Four HEPscreen Pilot Studies screening for chronic viral hepatitis in migrant populations. EU-HEP-
SCREEN, Project No 20101105. 2014. Available at:
http://hepscreen.eu/wp-content/uploads/2014/12/HEPscreen_Final-
WP6-report_Pilot-studies.pdf.
272. Jafferbhoy H, Miller MH, McIntyre P, Dillon JF. The effectiveness of outreach testing for hepatitis C in an immigrant
Pakistani population. Epidemiology and infection. 2012;140:1048-53.
273. Perumalswami PV, DeWolfe Miller F, Orabee H, Regab A, Adams M, Kapelusznik L, et al. Hepatitis C screening beyond CDC
guidelines in an Egyptian immigrant community. Liver international: Official Journal of the International Association for the
Study of the Liver. 2014;34:253-8.
274. Perumalswami PV, Factor SH, Kapelusznik L, Friedman SL, Pan CQ, Chang C, et al. Hepatitis Outreach Network: a practical
strategy for hepatitis screening with linkage to care in foreign-born communities. Journal of Hepatology. 2013;58:890-7.
275. Zuure FR, Bouman J, Martens M, Vanhommerig JW, Urbanus AT, Davidovich U, et al. Screening for hepatitis B and C in
first-generation Egyptian migrants living in the Netherlands. Liver International. 2013;33:727-38.

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
64
276. Falla AM, Rossi MK, Thomson R, Fernandez M, Cayla J, Csohán A, et al. Screening for chronic hepatitis B and C among
migrants: outcomes and costs of different screening models. European Scientific Conference on Applied Infectious Disease
Epidemiology (ESCAIDE) 2015.
277. Linde AC, Sweet KA, Nelson K, Mamo B, Chute SM. Impact of the Hepatitis Testing and Linkage to Care (HepTLC) Initiative
on Linkage to Care for Minnesota Refugees with Hepatitis B, 2012-2014. Public health reports (Washington, DC: 1974).
2016;131 Suppl 2:112-8.
278. Bottero J, Boyd A, Gozlan J, Carrat F, Nau J, Pauti M-D, et al. Simultaneous Human Immunodeficiency Virus-Hepatitis B-
Hepatitis C Point-of-Care Tests Improve Outcomes in Linkage-to-Care: Results of a Randomized Control Trial in Persons
Without Healthcare Coverage. Open Forum Infectious Diseases. 2015;2:162.
279. Hepatitis C Screening (NCEC National Clinical Guideline No. 15). Department of Health (Ireland), 2017.
280. Public Health England. Hepatitis C: migrant health guide: London: PHE, 2017. Available from:
https://www.gov.uk/guidance/hepatitis-c-migrant-health-guide#testing
.
281. Population à dépister et modalités du dépistage. Recommandations du comité d’experts réuni par l’Anaes. Agence nationale
d’accréditation et d’évaluation en santé. Dépistage de l’hépatite C - 2000. Haute autorité de santé: 2000 Available at:
https://
www.has-sante.fr/portail/jcms/c_271987/fr/depistage-de-l-hepatite-c-populations-a-depister-et-modalites-du-
depistage-recommandations-du-comite-d-experts-reuni-par-l-anaes.
282. Dhumeaux Daniel DJ-F, Patrick Y. Prise en charge thérapeutique et suivi de l’ensemble des personnes infectées par le virus
de l’hépatite C - Rapport de recommandations 2016. Conseil national du SIDA; Agence nationale de recherche sur le SIDA
et les hepatites virales (France), October 2016. Available at: https://solidarites-sante.gouv.fr/IMG/pdf/rapport_.pdf.
283. Hotez PJ, Brindley PJ, Bethony JM, King CH, Pearce EJ, Jacobson J. Helminth infections: the great neglected tropical
diseases. Journal of Clinical Investigation. 2008;118(4):1311-21.
284. Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291
diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet.
2012;380(9859):2197-223.
285. Puthiyakunnon S, Boddu S, Li Y, Zhou X, Wang C, Li J, et al. Strongyloidiasis--an insight into its global prevalence and
management. PLoS Negl Trop Dis. 2014;8(8):e3018.
286. Berry A, Paris L, Boissier J, Caumes E. Schistosomiasis Screening of Travelers to Corsica, France. Emerging Infectious
Diseases. 2016;22(1):159.
287. King CH. Parasites and poverty: the case of schistosomiasis. Acta Trop. 2010;113(2):95-104.
288. Zoni AC, Catalá L, Ault SK. Schistosomiasis Prevalence and Intensity of Infection in Latin America and the Caribbean
Countries, 1942-2014: A Systematic Review in the Context of a Regional Elimination Goal. PLoS Neglected Tropical
Diseases. 2016;10(3):e0004493.
289. Colley DG, Bustinduy AL, Secor WE, King CH. Human schistosomiasis. The Lancet. 2014;383(9936):2253-64.
290. World Health Organization. Strongyloidiasis (Fact sheet). WHO. 2016. Available at:
http://www.who.int/intestinal_worms/epidemiology/strongyloidiasis/en
.
291. González A, Gallo M, Valls ME, Muñoz J, Puyol L, Pinazo MJ, et al. Clinical and epidemiological features of 33 imported
Strongyloides stercoralis infections. Transactions of the Royal Society of Tropical Medicine and Hygiene. 2010;104(9):613-6.
292. Requena-Mendez A, Chiodini P, Bisoffi Z, Buonfrate D, Gotuzzo E, Munoz J. The laboratory diagnosis and follow up of
strongyloidiasis: a systematic review. PLoS Negl Trop Dis. 2013;7(1):e2002.
293. Buonfrate D, Requena-Mendez A, Angheben A, Munoz J, Gobbi F, Van Den Ende J, et al. Severe strongyloidiasis: a
systematic review of case reports. BMC Infect Dis. 2013;13:78.
294. Deniaud F, Rouesse C, Collignon A, Domingo A, Rigal L. [Failure to offer parasitology screening to vulnerable migrants in
France: Epidemiology and consequences]. Sante. 2010;20(4):201-8.
295. Hotez PJ, Alvarado M, Basanez MG, Bolliger I, Bourne R, Boussinesq M, et al. The global burden of disease study 2010:
interpretation and implications for the neglected tropical diseases. PLoS Negl Trop Dis. 2014;8(7):e2865.
296. Beltrame A, Buonfrate D, Gobbi F, Angheben A, Marchese V, Monteiro GB, et al. The hidden epidemic of schistosomiasis in
recent African immigrants and asylum seekers to Italy. Eur J Epidemiol. 2017.
297. Khan K, Sears J, Chan A, Rashid M, Greenaway C, Stauffer W, et al. Strongyloides and Schistosoma: evidence review for newly
arriving immigrants and refugee. The Canadian Collaboration for Immigrant and Refugee Health Appendix 8: Intestinal parasites
2011. Available at: http://www.cmaj.ca/content/suppl/2010/06/07/cmaj.090313.DC1/imm-para-8-at.pdf
298. Public Health England. Helminth infections: migrant health guide. London: PHE, 2017.
299. Chaves NJ, Paxton G, Biggs BA, Thambiran A, Smith M, Williams J. Recommendations for comprehensive post-arrival health
assessment for people from refugee-like backgrounds. Surry Hills. Australia: Australasian Society for Infectious Diseases
and Refugee Health Network, 2016.
300. Chaves NJ, Paxton GA, Biggs BA, Thambiran A, Gardiner J, Williams J, et al. The Australasian Society for Infectious
Diseases and Refugee Health Network of Australia recommendations for health assessment for people from refugee-like
backgrounds: an abridged outline. Med J Aust. 2017;206(7):310-5.
301. Ochodo EA, Gopalakrishna G, Spek B, Reitsma JB, van Lieshout L, Polman K, et al. Circulating antigen tests and urine
reagent strips for diagnosis of active schistosomiasis in endemic areas. Cochrane Database of Systematic Reviews. 2015(3).
302. King CH, Bertsch D. Meta-analysis of Urine Heme Dipstick Diagnosis of Schistosoma haematobium Infection, Including Low-
Prevalence and Previously-Treated Populations. PLoS Negl Trop Dis. 2013;7(9):e2431.
303. Wang W, Li Y, Li H, Xing Y, Qu G, Dai J, et al. Immunodiagnostic efficacy of detection of Schistosoma japonicum human
infections in China: a meta analysis. Asian Pacific Journal of Tropical Medicine. 2012;5(1):15-23.
304. Danso-Appiah A, Olliaro PL, Donegan S, Sinclair D, Utzinger J. Drugs for treating Schistosoma mansoni infection. Cochrane
Database of Systematic Reviews. 2013(2).
305. Kramer CV, Zhang F, Sinclair D, Olliaro PL. Drugs for treating urinary schistosomiasis. Cochrane Database Syst Rev.
2014(8):CD000053.
306. Pérez del Villar L, Burguillo FJ, López-Abán J, Muro A. Systematic Review and Meta-Analysis of Artemisinin Based Therapies
for the Treatment and Prevention of Schistosomiasis. PLoS ONE. 2012;7(9):e45867.
307. Yang F, Tan XD, Liu B, Yang C, Ni ZL, Gao XD, et al. Meta-analysis of the diagnostic efficiency of the questionnaires
screening for schistosomiasis. Parasitol Res. 2015;114(9):3509-19.

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
65
308. Campo Polanco L, Gutierrez LA, Cardona Arias J. [Diagnosis of Strongyloides Stercoralis infection: meta-analysis on
evaluation of conventional parasitological methods (1980-2013)]. Rev Esp Salud Publica. 2014;88(5):581-600.
309. Henriquez-Camacho C, Gotuzzo E, Echevarria J, White Jr AC, Terashima A, Samalvides F, et al. Ivermectin versus
albendazole or thiabendazole for Strongyloides stercoralis infection. Cochrane Database of Systematic Reviews. 2016(1).
310. Danso-Appiah A, Minton J, Boamah D, Otchere J, Asmah RH, Rodgers M, et al. Accuracy of point-of-care testing for
circulatory cathodic antigen in the detection of schistosome infection: systematic review and meta-analysis. Bull World
Health Organ. 2016;94(7):522-33A.
311. Kinkel HF, Dittrich S, Baumer B, Weitzel T. Evaluation of eight serological tests for diagnosis of imported schistosomiasis.
Clin Vaccine Immunol. 2012;19(6):948-53.
312. Lodh N, Mwansa JC, Mutengo MM, Shiff CJ. Diagnosis of Schistosoma mansoni without the stool: comparison of three
diagnostic tests to detect Schistosoma [corrected] mansoni infection from filtered urine in Zambia. Am J Trop Med Hyg.
2013;89(1):46-50.
313. Espirito-Santo MC, Alvarado-Mora MV, Dias-Neto E, Botelho-Lima LS, Moreira JP, Amorim M, et al. Evaluation of real-time
PCR assay to detect Schistosoma mansoni infections in a low endemic setting. BMC Infect Dis. 2014;14:558.
314. da Frota SM, Carneiro TR, Queiroz JA, Alencar LM, Heukelbach J, Bezerra FS. Combination of Kato-Katz faecal examinations
and ELISA to improve accuracy of diagnosis of intestinal schistosomiasis in a low-endemic setting in Brazil. Acta Trop.
2011;120 Suppl 1:S138-41.
315. Silveira AM, Costa EG, Ray D, Suzuki BM, Hsieh MH, Fraga LA, et al. Evaluation of the CCA Immuno-Chromatographic Test
to Diagnose Schistosoma mansoni in Minas Gerais State, Brazil. PLoS Negl Trop Dis. 2016;10(1):e0004357.
316. Espirito-Santo MC, Sanchez MC, Sanchez AR, Alvarado-Mora MV, Castilho VL, Goncalves EM, et al. Evaluation of the
sensitivity of IgG and IgM ELISA in detecting Schistosoma mansoni infections in a low endemicity setting. Eur J Clin
Microbiol Infect Dis. 2014;33(12):2275-84.
317. Bisoffi Z, Buonfrate D, Sequi M, Mejia R, Cimino RO, Krolewiecki AJ, et al. Diagnostic accuracy of five serological tests for
Strongyloides stercoralis infection. PLoS Negl Trop Dis. 2014;8(1):e2640.
318. Rascoe LN, Price C, Shin SH, McAuliffe I, Priest JW, Handali S. Development of Ss-NIE-1 recombinant antigen based assays
for immunodiagnosis of strongyloidiasis. PLoS Negl Trop Dis. 2015;9(4):e0003694.
319. Knopp S, Becker SL, Ingram KJ, Keiser J, Utzinger J. Diagnosis and treatment of schistosomiasis in children in the era of
intensified control. Expert Rev Anti Infect Ther. 2013;11(11):1237-58.
320. King CH, Olbrych SK, Soon M, Singer ME, Carter J, Colley DG. Utility of Repeated Praziquantel Dosing in the Treatment of
Schistosomiasis in High-Risk Communities in Africa: A Systematic Review. PLoS Negl Trop Dis. 2011;5(9):e1321.
321. Muennig P, Pallin D, Sell RL, Chan M-S. The Cost Effectiveness of Strategies for the Treatment of Intestinal Parasites in
Immigrants. New England Journal of Medicine. 1999;340(10):773-9.
322. Muennig P, Pallin D, Challah C, Khan K. The cost-effectiveness of ivermectin vs. albendazole in the presumptive treatment
of strongyloidiasis in immigrants to the United States. Epidemiology and Infection. 2004;132(6):1055-63.
323. Maskery B, Coleman MS, Weinberg M, Zhou W, Rotz L, Klosovsky A, et al. Economic Analysis of the Impact of Overseas and
Domestic Treatment and Screening Options for Intestinal Helminth Infection among US-Bound Refugees from Asia. PLoS
Negl Trop Dis. 2016;10(8):e0004910.
324. Worrell CM, Bartoces M, Karanja DM, Ochola EA, Matete DO, Mwinzi PN, et al. Cost analysis of tests for the detection of
Schistosoma mansoni infection in children in western Kenya. Am J Trop Med Hyg. 2015;92(6):1233-9.
325. Libman MD, MacLean JD, Gyorkos TW. Screening for schistosomiasis, filariasis, and strongyloidiasis among expatriates
returning from the tropics. Clin Infect Dis. 1993;17(3):353-9.
326. Buonfrate D, Sequi M, Mejia R, Cimino RO, Krolewiecki AJ, Albonico M, et al. Accuracy of five serologic tests for the follow
up of Strongyloides stercoralis infection. PLoS neglected tropical diseases. 2015;9(2):e0003491.
327. Espirito-Santo MC, Alvarado-Mora MV, Pinto PL, Sanchez MC, Dias-Neto E, Castilho VL, et al. Comparative Study of the
Accuracy of Different Techniques for the Laboratory Diagnosis of Schistosomiasis Mansoni in Areas of Low Endemicity in
Barra Mansa City, Rio de Janeiro State, Brazil. Biomed Res Int. 2015;2015:135689.
328. Beltrame A, Guerriero M, Angheben A, Gobbi F, Requena-Mendez A, Zammarchi L, et al. Accuracy of parasitological and
immunological tests for the screening of human schistosomiasis in immigrants and refugees from African countries: An
approach with Latent Class Analysis. PLoS Neglected Tropical Diseases. 2017;11(6):e0005593.
329. Requena-Méndez A, Buonfrate D, Gomez-Junyent J, Zammarchi L, Bisoffi Z, Muñoz J. Evidence-based guidelines for
screening and management of strongyloidiasis in non-endemic countries. The American Journal of Tropical Medicine and
Hygiene. 2017;97(3):645-52.
330. Albonico M, Becker SL, Odermatt P, Angheben A, Anselmi M, Amor A, et al. StrongNet: an international network to improve
diagnostics and access to treatment for strongyloidiasis control. PLoS Neglected Tropical Diseases. 2016;10(9):e0004898.
331. Boussinesq M, Gardon J, Gardon-Wendel N, Chippaux J-P. Clinical picture, epidemiology and outcome of Loa-associated
serious adverse events related to mass ivermectin treatment of onchocerciasis in Cameroon. Filaria Journal. 2003;2(1):S4.
332. Garcia HH, Del Brutto OH, Peru CWGi. Antiparasitic treatment of neurocysticercosis-The effect of cyst destruction in seizure
evolution. Epilepsy & Behavior. 2017.
333. Vanijanonta S, Bunnag D. Treatment of cysticercosis with praziquantel at the Bangkok Hospital for Tropical Diseases. The
Southeast Asian Journal of Tropical Medicine and Public Health. 1985;16(3):435-40.
334. Atkins D, Best D, Briss PA, Eccles M, Falck-Ytter Y, Flottorp S, et al. Grading quality of evidence and strength of
recommendations. BMJ (Clinical research ed). 2004;328(7454):1490.
335. Update of laboratory medicine procedures related to the diagnosis of strongyloidiasis. French National Authority for Health
(HAS), April 2017.
336. Assessement of laboratory medicine procedures related to the diagnosis of schistosomiasis (bilharzia). French National
Authority for Health (HAS), January 2017.
337. World Health Organization. European Vaccine Action Plan 2015-2020. Copenhagen: WHO Regional Office for Europe, 2014.
338. Barnett ED, Christiansen D, Figueira M. Seroprevalence of measles, rubella, and varicella in refugees. Clin Infect Dis.
2002;35(4):403-8.
339. Greenaway C, Dongier P, Boivin JF, Tapiero B, Miller M, Schwartzman K. Susceptibility to measles, mumps, and rubella in
newly arrived adult immigrants and refugees. Ann Intern Med. 2007;146(1):20-4.

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
66
340. Toikkanen SE, Baillot A, Dreesman J, Mertens E. Seroprevalence of Antibodies against Measles, Rubella and Varicella
among Asylum Seekers Arriving in Lower Saxony, Germany, November 2014-October 2015. Int J Environ Res Public Health.
2016;13(7).
341. Freidl GS, Tostmann A, Curvers M, Ruijs WLM, Smits G, Schepp R, et al. Immunity against measles, mumps, rubella,
varicella, diphtheria, tetanus, polio, hepatitis A and hepatitis B among adult asylum seekers in the Netherlands, 2016.
Vaccine. 2018;36(12):1664-72.
342. Ceccarelli G, Vita S, Riva E, Cella E, Lopalco M, Antonelli F, et al. Susceptibility to measles in migrant population: implication
for policy makers. Journal of Travel Medicine. 2018;25(1).
343. Nakken CS, Skovdal M, Nellums LB, Friedland JS, Hargreaves S, Norredam M. Vaccination status and needs of asylum-
seeking children in Denmark: a retrospective data analysis. Public Health. 2018;158:110-6.
344. Hübschen JM, Charpentier E, Weicherding P, Muller CP. IgG antibody prevalence suggests high immunization needs in
newcomers to Luxembourg, 2012. Vaccine. 2018;36(6):899-905.
345. Roberton T, Weiss W, Doocy S, Team JHAS, Team LHAS. Challenges in estimating vaccine coverage in refugee and
displaced populations: results from household surveys in Jordan and Lebanon. Vaccines. 2017;5(3):22.
346. Filia A, Amendola A, Faccini M, Del Manso M, Senatore S, Bianchi S, et al. Outbreak of a new measles B3 variant in the
Roma/Sinti population with transmission in the nosocomial setting, Italy, November 2015 to April 2016. Euro Surveill.
2016;21(20).
347. Williams GA, Bacci S, Shadwick R, Tillmann T, Rechel B, Noori T, et al. Measles among migrants in the European Union and
the European Economic Area. Scand J Public Health. 2016;44(1):6-13.
348. Jones G, Haeghebaert S, Merlin B, Antona D, Simon N, Elmouden M, et al. Measles outbreak in a refugee settlement in
Calais, France: January to February 2016. Euro Surveill. 2016;21(11):30167.
349. Khetsuriani N, Perehinets I, Nitzan D, Popovic D, Moran T, Allahverdiyeva V, et al. Responding to a cVDPV1 outbreak in
Ukraine: Implications, challenges and opportunities. Vaccine. 35(36): 2017.
350. Werber D, Hoffmann A, Santibanez S, Mankertz A, Sagebiel D. Large measles outbreak introduced by asylum seekers and
spread among the insufficiently vaccinated resident population, Berlin, October 2014 to August 2015. Euro Surveill.
2017;22(34).
351. Derrough T, Salekeen A. Lessons learnt to keep Europe polio-free: a review of outbreaks in the European Union, European
Economic Area, and candidate countries, 1973 to 2013. Euro Surveill. 2016;21(16).
352. Woudenberg T, van Binnendijk RS, Sanders EAM, Wallinga J, de Melker HE, Ruijs WLM, et al. Large measles epidemic in
the Netherlands, May 2013 to March 2014: changing epidemiology. Euro Surveill. 2017;22(3).
353. Antona D, Lévy-Bruhl D, Baudon C, Freymuth F, Lamy M, Maine C, et al. Measles elimination efforts and 2008–2011
outbreak, France. Emerging Infectious Diseases. 2013;19(3):357.
354. Hargreaves s NL, Ramsay M, et al. Who is responsible for the vaccination of migrants in Europe? The Lancet Infectious
Diseases. 2018;391.
355. World Health Organization. Immunization coverage 2018. Available at:
http://www.who.int/news-room/fact-
sheets/detail/immunization-coverage.
356. World Health Organization. Global Health Observatory data repository: Immunization: WHO [19 July 2018]. Available at:
http://apps.who.int/gho/data/view.main.uhcimmunization
357. Anderson RM. The concept of herd immunity and the design of community-based immunization programmes. Vaccine.
1992;10(13):928-35.
358. Plotkin, SA. In: Orenstein WA, Offit PA, Edwards KM, editors. Plotkin's Vaccines (Seventh Edition): Elsevier; 2018. p. iv.
359. Bica MA, Clemens R. Vaccination policies of immigrants in the EU/EEA Member States-the measles immunization example.
European Journal of Public Health. 2018;28(3):439-44.
360. De Vito E, Parente P, De Waure C, Poscia A, Ricciardi W. A review of evidence on equitable delivery, access and utilization
of immunization services for migrants and refugees in the WHO European Region. 2017. Available at:
http://www.euro.who.int/__data/assets/pdf_file/0005/351644/HEN53.pdf
.
361. European Centre for Disease Prevention and Control. Diptheria. In: ECDC. Annual epidemiological report for 2015.
Stockoholm: ECDC; 2017.
362. European Centre for Disease Prevention and Control. Risk of measles transmission in the EU/EEA, 21 March 2018.
Stockholm: ECDC; 2018.
363. European Centre for Disease Prevention and Control. Pertussis. In: ECDC. Annual epidemiological report for 2015.
Stockholm: ECDC; 2017.
364. European Centre for Disease Prevention and Control. Tetanus. In: ECDC. Annual epidemiological report for 2015.
Stockholm: ECDC; 2017.
365. European Centre for Disease Prevention and Control. Haemophilus influenzae. In: ECDC. Annual epidemiological report for
2015. Stockholm: ECDC; 2017.
366. European Centre for Disease Prevention and Control. Bi-annual measles and rubella monitoring report, October 2017.
ECDC: Stockholm, 2017. Available at: https://ecdc.europa.eu/sites/portal/files/documents/Bi-
annual%20measles%20rubella%20monitoring-OCT-2017.pdf.
367. Adam IF, Nakamura K, Kizuki M, Al Rifai R, Vanching U. Relationship between implementing interpersonal communication
and mass education campaigns in emergency settings and use of reproductive healthcare services: evidence from Darfur,
Sudan. BMJ Open. 2015;5(9):e008285.
368. Hu Y, Luo S, Tang X, Lou L, Chen Y, Guo J, et al. Does introducing an immunization package of services for migrant
children improve the coverage, service quality and understanding? An evidence from an intervention study among 1548
migrant children in eastern China. BMC Public Health. 2015;15:664.
369. Milne B, Raman S, Thomas P, Shah S. Immunisation of refugee and migrant young people: can schools do the job? Aust N
Z J Public Health. 2006;30(6):526-8.
370. Ndiaye SM, Ahmed MA, Denson M, Craig AS, Kretsinger K, Cherif B, et al. Polio outbreak among nomads in Chad: outbreak
response and lessons learned. J Infect Dis. 2014;210 Suppl 1:S74-84.
371. Sengupta P, Benjamin AI, Myles PR, Babu BV. Evaluation of a community-based intervention to improve routine childhood
vaccination uptake among migrants in urban slums of Ludhiana, India. J Public Health (Oxf). 2016.

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
67
372. Sheikh MA, Makokha F, Hussein AM, Mohamed G, Mach O, Humayun K, et al. Combined use of inactivated and oral
poliovirus vaccines in refugee camps and surrounding communities - Kenya, December 2013. MMWR Morb Mortal Wkly
Rep. 2014;63(11):237-41.
373. Spadea A, Semyonov L, Unim B, Giraldi G, Corda B, D'Amici AM, et al. Action against vaccine-preventable infectious
diseases and tuberculosis in Nomad Camps: the experience of a Local Health Unit in Rome. Ann Ig. 2014;26(2):176-80.
374. Kaji A, Parker DM, Chu CS, Thayatkawin W, Suelaor J, Charatrueangrongkun R, et al. Immunization coverage in migrant
school children along the Thailand-Myanmar border. Journal of Immigrant and Minority Health. 2016;18(5):1038-45.
375. Fang H, Yang L, Zhang H, Li C, Wen L, Sun L, et al. Strengthening health system to improve immunization for migrants in
China. International Journal for Equity in Health. 2017;16(1):19.
376. Brockmann SO, Wjst S, Zelmer U, Carollo S, Schmid M, Roller G, et al. ÖGD-Initiative zur Verbesserung der Durchimpfung
bei Asylsuchenden. Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz. 2016;59(5):592-8.
377. Cohen AL, Veenstra D. Economic analysis of prevaccination serotesting compared with presumptive immunization for polio,
diphtheria, and tetanus in internationally adopted and immigrant infants. Pediatrics. 2006;117(5):1650-5.
378. Coleman MS, Burke HM, Welstead BL, Mitchell T, Taylor EM, Shapovalov D, et al. Cost analysis of measles in refugees
arriving at Los Angeles International Airport from Malaysia. Human Vaccines & Immunotherapeutics. 2017;13(5):1084-90.
379. Joo H, Maskery B, Mitchell T, Leidner A, Klosovsky A, Weinberg M. A comparative cost analysis of the Vaccination Program
for US-bound Refugees. Vaccine. 2018;36(20):2896-901.
380. Agudelo-Suárez AA, Gil-González D, Vives-Cases C, Love JG, Wimpenny P, Ronda-Pérez E. A metasynthesis of qualitative
studies regarding opinions and perceptions about barriers and determinants of health services' accessibility in economic
migrants. BMC Health Serv Res. 2012;12:461.
381. Ingleby, D. and Petrova-Benedict, R. (2016) Recommendations on access to health services for migrants in an irregular
situation: an expert consensus. Brussels: International Organization for Migration (IOM) Regional Office Brussels, Migration
Health Division. Available at: http://equi-health.eea.iom.int/index.php/9-uncategorised/336-expert-consensus
.
382. Baker DL, Dang MT, Ly MY, Diaz R. Perception of barriers to immunization among parents of Hmong origin in California.
American Journal of Public Health. 2010;100(5):839-45.
383. Harmsen IA, Bos H, Ruiter RAC, Paulussen TGW, Kok G, de Melker HE, et al. Vaccination decision-making of immigrant
parents in the Netherlands; a focus group study. BMC Public Health. 2015;15:1229.
384. Canavati S, Plugge E, Suwanjatuporn S, Sombatrungjaroen S, Nosten F. Barriers to immunization among children of migrant
workers from Myanmar living in Tak province, Thailand. Bulletin of the World Health Organization. 2011;89(7):528-31.
385. Kowal SP, Jardine CG, Bubela TM. "If they tell me to get it, I'll get it. If they don't...": Immunization decision-making
processes of immigrant mothers. Can J Public Health. 2015;106(4):e230-5.
386. Wang LDL, Lam WWT, Wu JT, Liao Q, Fielding R. Chinese immigrant parents' vaccination decision making for children: a
qualitative analysis. BMC Public Health. 2014;14:133.
387. Devroey D, Riffi A, Balemans R, Van De Vijver E, Chovanova H, Vandevoorde J. Comparison of knowledge and attitudes
about vaccination between Belgian and immigrant adolescents. Journal of Infection and Public Health. 2013;6(1):1-9.
388. Guttmann A, Manuel D, Stukel TA, Desmeules M, Cernat G, Glazier RH. Immunization coverage among young children of
urban immigrant mothers: findings from a universal health care system. Ambul Pediatr. 2008;8(3):205-9.
389. Hargreaves S, Nellums L, Ramsay M, Saliba V, Majeem A, Mounier-Jack S, et al. Who is responsible for the vaccination of
migrants in Europe? The Lancet. 2018;391.
390. World Health Organization. Vaccination in acute humanitarian emergencies: a framework for decision making: WHO; 2017
[19 July 2018]. Available from: http://apps.who.int/iris/bitstream/10665/255575/1/WHO-IVB-17.03-eng.pdf
.
391. Bozorgmehr K, Samuilova M, Petrova-Benedict R, Girardi E, Piselli P, Kentikelenis A. Infectious disease health services for
refugees and asylum seekers during a time of crisis: A scoping study of six European Union countries. Health Policy
(Amsterdam, Netherlands). 2018.
392. Giambi C, Del Manso M, Dalla Zuanna T, Riccardo F, Bella A, Caporali MG, et al. National immunization strategies targeting
migrants in six European countries. Vaccine. 2018.
393. Linee Guida Salute Migranti. I controlli alla frontiera. La frontiera dei controlli. Controlli sanitari all'arrivo e percorsi di tutela
per i migranti ospiti nei centri di accoglienza. 2017.
394. Guidelines for evaluating and updating immunizations during the domestic medical examination for newly arrived refugees.
U.S. Department of Health and Human Services, US Centers for Disease Control and Prevention; 2015.
395. US CDC. Recommended Immunizations for Adults by Age in Easy-to-read Format: US Centers for Disease Control and
Prevention; 2018. Available at: https://www.cdc.gov/vaccines/schedules/easy-to-read/adult-easyread.html
.
396. US CDC. 2018 Recommended Immunizations For Infants and Children (Birth through 6 Years) in Easy-to-read Format: US
Centers for Disease Control and Prevention; 2018 [19 July 2018]. Available at:
https://www.cdc.gov/vaccines/schedules/easy-to-read/child-easyread.html
.
397. Simmons R, Ireland G, Irving W, Hickman M, Sabin C, Ijaz S, et al. Establishing the cascade of care for hepatitis C in
England—benchmarking to monitor impact of direct acting antivirals. Journal of Viral Hepatitis. 2018.
398. Anderson LF, Tamne S, Watson JP, Cohen T, Mitnick C, Brown T, et al. Treatment outcome of multi-drug resistant
tuberculosis in the United Kingdom: retrospective-prospective cohort study from 2004 to 2007. Eurosurveillance.
2013;18(40):20601.
399. Coppola N, Alessio L, Gualdieri L, Pisaturo M, Sagnelli C, Minichini C, et al. Hepatitis B virus infection in undocumented immigrants
and refugees in Southern Italy: demographic, virological, and clinical features. Infectious Diseases of Poverty. 2017;6(1):33.
400. Ross J, Cunningham CO, Hanna DB. HIV outcomes among migrants from low-income and middle-income countries living in
high-income countries: a review of recent evidence. Current Opinion in Infectious Diseases. 2018;31(1):25-32.
401. Nellums LB, Rustage K, Hargreaves S, Friedland JS. Multidrug-resistant tuberculosis treatment adherence in migrants: a
systematic review and meta-analysis. BMC Medicine. 2018;16(1):27.
402. Stanicole AE, Huber M. Access to Health Care for Migrants, Ethnic Minorities, and Asylum Seekers in Europe. Vienna:
European Centre for Social Welfare Policy and Research; 2009.
403. van Loenen T, van den Muijsenbergh M, Hofmeester M, Dowrick C, van Ginneken N, Mechili EA, et al. Primary care for
refugees and newly arrived migrants in Europe: a qualitative study on health needs, barriers and wishes. European Journal
of Public Health. 2018;28(1):82-7.

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
68
404. Aldridge RW, Miller AK, Jakubowski B, et al. Falling through the Cracks: The Failure of Universal Healthcare Coverage in
Europe, European Network to Reduce Vulnerabilities in Health Observatory Report. London 2017.
405. Singer M, Bulled N, Ostrach B, Mendenhall E. Syndemics and the biosocial conception of health. The Lancet.
2017;389(10072):941-50.
406. Seedat F, Hargreaves S, Friedland JS. Engaging New Migrants in Infectious Disease Screening: A Qualitative Semi-
Structured Interview Study of UK Migrant Community Health-Care Leads. PLOS ONE. 2014;9(10):e108261.
407. van den Muijsenbergh M, van Weel-Baumgarten E, Burns N, O'Donnell C, Mair F, Spiegel W, et al. Communication in cross-
cultural consultations in primary care in Europe: the case for improvement. The rationale for the RESTORE FP 7 project.
Primary Health Care Research & Development. 2013;15(2):122-33.
408. O'Reilly de Brún M, Brún T, O'Donnell CA, et al. Material practices for meaningful engagement: An analysis of participatory
learning and action research techniques for data generation and analysis in a health research partnership. Health
Expectations. 2018;21(1):159-70.
409. Lionis C, Papadakaki M, Saridaki A, Dowrick C, O'Donnell CA, Mair FS, et al. Engaging migrants and other stakeholders to
improve communication in cross-cultural consultation in primary care: a theoretically informed participatory study. BMJ
Open. 2016;6(7).
410. Pareek M. NIHR: Impact, acceptability and cost-effectiveness of identifying infectious diseases amongst migrants in primary
care. London: NIHR; 2016.

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
69
Annex 1. Top ten countries of birth of
immigrants to the EU/EEA (average of 2014,
2015 and 2016)
EU/EEA*
Austria
Belgium
Total
1 226 859
%
Total
64 258
%
Total
59 971
%
Syria
94 356
8
Syria
11 745
18
Morocco
6 310
11
China
83 883
7
Afghanistan
9 158
14
Syria
5 800
10
India
77 002
6
Serbia
5 693
9
Afghanistan
3 629
6
Morocco
50 469
4
Bosnia & H.
4 986
8
Iraq
3 616
6
United States
43 132
4
Iraq
3 746
6
India
2 324
4
Pakistan
35 764
3
Turkey
2 895
5
DR Congo
2 154
4
Ukraine
35 384
3
Iran
2 829
4
United States
2 142
4
Moldova
29 606
2
Russia
2 178
3
Turkey
2 087
3
Russia
24 976
2
Ukraine
1 415
2
Cameroon
1 603
3
Brazil
24 915
2
China
1 359
2
China
1 398
2
Other
727 371
59
Other
18 255
28
Other
28 908
48
Bulgaria
Czech Republic
Croatia
Total
12 373
%
Total
17 464
%
Total
7 242
%
Syria
3 563
29
Ukraine
5 643
32
Bosnia & H.
4 656
64
Russia
3 234
26
Russia
1 571
9
Serbia
674
9
Turkey
1 314
11
United States
1 267
7
Kosovo
308
4
Ukraine
1 122
9
Vietnam
1 252
7
FYR Macedonia
268
4
FYR Macedonia
351
3
Moldova
989
6
Russia
160
2
Kazakhstan
298
2
Mongolia
593
3
Ukraine
135
2
Serbia
233
2
India
466
3
United States
128
2
Moldova
225
2
Kazakhstan
416
2
China
89
1
United States
198
2
Turkey
315
2
Switzerland
86
1
China
184
1
China
314
2
Montenegro
56
1
Other
1 652
13
Other
4 639
27
Other
682
9
Denmark
Estonia
Finland
Total
30 996
%
Total
3 531
%
Total
16 384
%
Syria
9 228
29
Russia
1 371
39
Iraq
1 613
10
India
1 549
26
Ukraine
931
26
Russia
987
6
Philippines
1 361
11
Belarus
116
3
Syria
930
6
China
1 307
9
United States
110
3
China
775
5
Eritrea
1 284
3
India
72
2
India
772
5
United States
1 279
2
Georgia
72
2
Afghanistan
708
4
Ukraine
1 251
2
Nigeria
72
2
Vietnam
703
4
Greenland
954
2
Kazakhstan
68
2
Somalia
638
4
Iran
947
2
Turkey
55
2
Thailand
566
3
Nepal
768
1
China
48
1
Iran
563
3
Other
11 067
13
Other
617
17
Other
8 128
50

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
70
Hungary
Iceland
Italy
Total
25 465
%
Total
1 047
%
Total
201 426
%
Ukraine
8 326
29
United
States
162
16
Morocco
15 600
8
Serbia
3 555
26
Philippines
78
7
China
13 446
7
China
3 230
11
Thailand
51
5
Bangladesh
11 871
6
United States
1 108
9
Vietnam
47
5
Pakistan
11 837
6
Russia
637
3
China
44
4
Albania
11 618
6
Turkey
617
2
Syria
37
4
India
10 711
5
Iran
511
2
Canada
34
3
Brazil
9 986
5
Japan
488
2
Ukraine
31
3
Nigeria
9 311
5
India
483
2
Russia
29
3
Egypt
7 549
4
South Korea
362
1
Serbia
27
3
Senegal
7 345
4
Other
6 146
13
Other
506
48
Other
92 151
46
Latvia
Liechtenstein
Lithuania
Total
3 365
%
Total
332
%
Total
5 213
%
Russia
1 511
45
Switzerland
195
59
Ukraine
1 656
32
Ukraine
689
20
Brazil
18
5
Russia
1 391
27
Belarus
391
12
Turkey
10
3
Belarus
757
15
Uzbekistan
143
4
Ukraine
9
3
India
147
3
Kazakhstan
85
3
China
8
3
Kazakhstan
139
3
China
62
2
Syria
7
2
Georgia
114
2
Philippines
53
2
Bosnia & H.
7
2
Moldova
107
2
India
51
2
Dominican
Rep.
6
2
Azerbaijan
84
2
United States
44
1
Kosovo
5
2
Iran
69
1
Azerbaijan
38
1
Philippines
5
2
United
States
65
1
Other
298
9
Other
62
19
Other
683
13
Luxembourg
Norway
Romania
Total
7 084
%
Total
31 279
%
Total
32 920
%
United States
580
8
Syria
6 016
19
Moldova
23 282
71
China
436
6
Eritrea
2 659
9
Ukraine
2 166
7
Syria
382
5
Philippines
2 166
7
Turkey
673
2
Cape Verde
339
5
Somalia
1 469
5
China
559
2
India
330
5
India
1 407
4
Israel
457
1
Brazil
302
4
Afghanistan
1 239
4
Russia
363
1
Russia
288
4
Thailand
1 195
4
Syria
358
1
Morocco
239
3
United
States
1 003
3
Serbia
349
1
Iraq
225
3
China
783
3
United
States
349
1
Serbia
183
3
Pakistan
714
2
Iraq
347
1
Other
3 781
53
Other
12 626
40
Other
4 019
12
Slovakia
Slovenia
Spain
Total
1 178
%
Total
10 443
%
Total
224 131
%
Ukraine
365
31
Bosnia & H.
4 513
43
Morocco
24 661
11
United States
100
9
Kosovo
1 533
15
Venezuela
20 462
9
Serbia
87
7
Serbia
1 445
14
Colombia
15 404
7
Switzerland
69
6
FYR Macedonia
1 199
11
China
9 527
4
Russia
61
5
Russia
543
5
Argentina
8 897
4
Iraq
52
4
Ukraine
280
3
Dominica
8 829
4
Vietnam
31
3
United States
99
1
Brazil
8 762
4
Canada
30
3
China
92
1
Ecuador
8 513
4
China
29
2
Montenegro
82
1
Honduras
8 144
4
FYR Macedonia
24
2
Switzerland
38
0
Cuba
8 106
4
Other
331
28
Other
619
6
Other
102 826
46

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
71
Sweden
United Kingdom
Total
94 774
%
Total
294 284
%
Syria
36 081
38
India
45 754
16
Eritrea
6 247
7
China
42 957
15
Iraq
4 125
4
United States
19 988
7
India
3 639
4
Pakistan
12 713
4
Afghanistan
3 339
4
Nigeria
8 842
3
China
2 514
3
Canada
8 770
3
Iran
2 337
2
South Africa
7 815
3
United States
1 639
2
Malaysia
7 305
2
Thailand
1 600
2
Thailand
7 182
2
Turkey
1 505
2
Saudi Arabia
6 820
2
Other
31 748
33
Other
126 139
43
Source: Eurostat migr_imm3ctb
Data disaggregated by all countries of birth are not available for Germany, Ireland, Greece, Spain, France, Cyprus, Malta, Poland,
Portugal, and the United Kingdom.
Spain and the UK submitted only data on major countries of birth. These are also included in this table.
Note: Some countries include asylum seekers in the total number of immigrants, others do not. The metadata do not allow for
the differentiation of national approaches.
Includes only 23 countries (see above), accounting for 56% of non-EU/EEA migrants. The figure for Syria would be far greater if
Germany were included.

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
72
Annex 2. Top ten origins (nationalities) of
asylum seekers in the EU/EEA (average of
applications in 2015, 2016 and 2017)
EU/EEA
Austria
Belgium
Total
1 037 378
%
Total
49 063
%
Total
22 240
%
Syria
270 728
26
Syria
13 538
28
Syria
5 052
23
Afghanistan
137 500
13
Afghanistan
13 295
27
Afghanistan
3 650
16
Iraq
99 930
10
Iraq
5 765
12
Iraq
3 525
16
Pakistan
41 447
4
Pakistan
2 250
5
Somalia
1 010
5
Albania
39 595
4
Iran
2 243
5
Guinea
702
3
Nigeria
38 535
4
Somalia
1 400
3
Unknown
685
3
Eritrea
31 682
3
Nigeria
1 342
3
Albania
643
3
Iran
28 159
3
Stateless
1 273
3
DR Congo
560
3
Kosovo
27 200
3
Russia
1 203
2
Russia
445
2
Russia
18 121
2
Kosovo
857
2
Eritrea
443
2
Other
304 482
29
Other
5 897
12
Other
5 525
25
Bulgaria
Croatia
Cyprus
Total
14 203
%
Total
1 032
%
Total
3,130
%
Afghanistan
5 287
37
Afghanistan
292
28
Syria
1 282
41
Iraq
4 368
31
Syria
167
16
India
240
8
Syria
3 160
22
Iraq
125
12
Vietnam
208
7
Pakistan
850
6
Pakistan
98
10
Pakistan
172
5
Iran
228
2
Iran
70
7
Bangladesh
153
5
Stateless
68
0
Algeria
63
6
Egypt
147
5
Sri Lanka
35
0
Turkey
50
5
Somalia
135
4
Ukraine
33
0
Morocco
35
3
Palestine
90
3
Bangladesh
33
0
Libya
17
2
Sri Lanka
88
3
Algeria
18
0
Bangladesh
15
1
Cameroon
68
2
Other
122
1
Other
100
10
Other
547
17
Czech Republic
Denmark
Estonia
Total
1 175
%
Total
9 902
%
Total
172
%
Ukraine
405
34
Syria
3 533
36
Syria
47
27
Syria
88
8
Afghanistan
1 165
12
Ukraine
37
21
Cuba
87
7
Iran
1 068
11
Iraq
13
8
Iraq
73
6
Stateless
765
8
Russia
13
8
Armenia
65
6
Eritrea
750
8
Georgia
8
5
Azerbaijan
58
5
Iraq
678
7
Afghanistan
7
4
Georgia
57
5
Morocco
267
3
Palestine
7
4
Vietnam
57
5
Somalia
197
2
Albania
5
3
Russia
40
3
Algeria
108
1
Iran
5
3
China
35
3
Libya
98
1
Armenia
5
3
Other
210
18
Other
1 272
13
Other
25
15

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
73
Finland
France
Germany
Total
13 863
%
Total
73 298
%
Total
451 675
%
Iraq
7 493
54
Albania
7 197
10
Syria
157 958
35
Afghanistan
2 060
15
Afghanistan
5 008
7
Afghanistan
58 272
13
Somalia
833
6
Syria
4 695
6
Iraq
49 277
11
Syria
738
5
Haiti
4 692
6
Albania
24 145
5
Albania
312
2
DR Congo
3 663
5
Iran
13 477
3
Iran
282
2
Kosovo
2 952
4
Eritrea
13 318
3
Eritrea
260
2
Guinea
2 938
4
Kosovo
13 233
3
Russia
245
2
Bangladesh
2 802
4
Unknown
12 597
3
Unknown
158
1
Iraq
2 672
4
Pakistan
8 785
2
Nigeria
137
1
Algeria
2 618
4
Nigeria
8 575
2
Other
1 345
10
Other
34 062
46
Other
92 038
20
Greece
Hungary
Iceland
Total
39 238
%
Total
68 413
%
Total
1 053
%
Syria
15 420
39
Syria
23 173
34
FYR
Macedonia
253
24
Pakistan
4 757
12
Afghanistan
19 233
28
Albania
240
23
Afghanistan
4 440
11
Kosovo
7 933
12
Georgia
165
16
Iraq
4 405
11
Pakistan
6 253
9
Iraq
90
9
Albania
1 520
4
Iraq
4 442
6
Syria
33
3
Bangladesh
948
2
Bangladesh
1 423
2
Pakistan
25
2
Iran
857
2
Iran
1 043
2
Somalia
25
2
Palestine
737
2
Unknown
512
1
Iran
23
2
Turkey
680
2
Palestine
407
1
Afghanistan
20
2
Georgia
622
2
Morocco
398
1
Nigeria
15
1
Other
4 853
12
Other
3 595
5
Other
165
16
Ireland
Italy
Latvia
Total
2 782
%
Total
109 563
%
Total
332
%
Pakistan
590
21
Nigeria
23 093
21
Syria
98
30
Syria
305
11
Pakistan
11 075
10
Vietnam
42
13
Albania
242
9
Gambia The
8 522
8
Iraq
32
10
Zimbabwe
185
7
Bangladesh
8 237
8
Afghanistan
28
9
Nigeria
183
7
Senegal
7 405
7
Russia
20
6
Georgia
140
5
Mali
6 415
6
Ukraine
18
6
Bangladesh
130
5
Côte d'Ivoire
6 300
6
Georgia
15
5
Afghanistan
105
4
Guinea
5 173
5
Eritrea
10
3
South Africa
87
3
Eritrea
4 822
4
Tajikistan
10
3
Iraq
75
3
Ghana
4 363
4
India
8
3
Other
740
27
Other
24 158
22
Other
50
15

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
74
Liechtenstein
Lithuania
Luxembourg
Total
60
%
Total
400
%
Total
2 172
%
Serbia
15
25
Syria
113
28
Syria
457
21
Ukraine
10
17
Russia
55
14
Iraq
288
13
Albania
5
8
Ukraine
42
10
Albania
160
7
Georgia
5
8
Afghanistan
25
6
Kosovo
150
7
Syria
5
8
Tajikistan
25
6
Eritrea
130
6
Somalia
5
8
Iraq
22
5
Serbia
128
6
Eritrea
5
8
Georgia
20
5
Afghanistan
107
5
Belarus
5
8
Belarus
20
5
Morocco
98
5
China
5
8
Armenia
15
4
Algeria
87
4
FYR Macedonia
0
0
Eritrea
10
3
Georgia
75
3
Other
0
0
Other
53
13
Other
492
23
Malta
Netherlands
Norway
Total
1 657
%
Total
25 757
%
Total
12 177
%
Libya
653
39
Syria
8 157
32
Syria
4 025
33
Syria
372
22
Eritrea
3 615
14
Afghanistan
2 470
20
Somalia
197
12
Iraq
1 605
6
Eritrea
1 390
11
Eritrea
130
8
Afghanistan
1 298
5
Iraq
1 093
9
Ukraine
63
4
Iran
1 163
5
Iran
503
4
Iraq
35
2
Albania
1 012
4
Stateless
460
4
Nigeria
18
1
Stateless
975
4
Ethiopia
298
2
Egypt
18
1
Morocco
777
3
Somalia
227
2
Venezuela
18
1
Algeria
638
2
Albania
213
2
Ethiopia
17
1
Serbia
518
2
Pakistan
163
1
Other
135
8
Other
5 998
23
Other
1 333
11
Poland
Portugal
Romania
Total
7 660
%
Total
842
%
Total
2 570
%
Russia
5 513
72
Ukraine
210
25
Iraq
1 113
43
Ukraine
823
11
DR Congo
75
9
Syria
758
30
Tajikistan
480
6
Angola
57
7
Afghanistan
140
5
Armenia
182
2
Guinea
43
5
Pakistan
123
5
Syria
122
2
Congo
40
5
Iran
80
3
Georgia
102
1
Mali
40
5
Turkey
43
2
Kyrgyzstan
57
1
Pakistan
37
4
Stateless
33
1
Vietnam
48
1
China
28
3
Eritrea
22
1
Iraq
45
1
Iraq
23
3
Palestine
20
1
Turkey
42
1
Sierra
Leone
23
3
Ukraine
18
1
Other
247
3
Other
265
31
Other
218
8

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
75
Slovakia
Slovenia
Spain
Total
158
%
Total
973
%
Total
20 058
%
Iraq
63
40
Afghanistan
343
35
Venezuela
4 957
25
Afghanistan
20
13
Syria
125
13
Syria
4 263
21
Ukraine
12
7
Pakistan
90
9
Ukraine
2 692
13
Pakistan
10
6
Algeria
77
8
Colombia
1 047
5
Syria
8
5
Iraq
60
6
Algeria
838
4
Vietnam
7
4
Turkey
55
6
Palestine
762
4
Iran
5
3
Iran
52
5
El Salvador
550
3
Cuba
5
3
Kosovo
30
3
Honduras
498
2
Unknown
5
3
Morocco
28
3
Morocco
413
2
Algeria
3
2
Eritrea
22
2
Cameroon
333
2
Other
20
13
Other
92
9
Other
3 705
18
Sweden
United
Kingdom
Total
66 540
%
Total
35 220
%
Syria
20 283
30
Iran
3 867
11
Afghanistan
14 860
22
Pakistan
3 422
10
Iraq
7 903
12
Iraq
3 215
9
Stateless
3 130
5
Afghanistan
2 627
7
Eritrea
2 932
4
Eritrea
2 048
6
Somalia
2 187
3
Albania
1 858
5
Iran
2 037
3
Bangladesh
1 852
5
Albania
1 327
2
Syria
1 720
5
Georgia
808
1
India
1 717
5
Ukraine
780
1
Nigeria
1 688
5
Other
10 293
15
Other
11 207
32
Source: Eurostat migr_asyappctza

Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants SCIENTIFIC ADVICE
76
Annex 3. Terms of reference of the ad hoc
scientific panel
Background
The European health policy framework ‘Health 2020’ aims to ‘significantly improve the health and well-being of
populations, reduce health inequalities, strengthen public health and ensure people-centred health systems that
are universal, equitable, sustainable and of high quality’. In the area of migrant health, ECDC will work towards this
aim by embarking on a project to develop evidence-based guidance for prevention of infectious diseases among
newly arrived migrants to the EU/EEA.
The objective of this project is to systematically review and synthesize the evidence on infectious diseases
considering emergency public health and longer-term preventive actions for newly arriving migrants within existing
EU/EEA health systems. Using the newly developed GRADE ‘evidence to decision’ framework, ECDC will search for
evidence and update high quality systematic reviews on effectiveness, acceptability, feasibility, equity, resource use
and cost effectiveness of migrant screening. This review will inform the deliberation of the evidence and
subsequent development of an evidence-based guidance document, which will serve as a European guidance for
key migrant health infectious diseases. A scientific panel will be set up to oversee the process.
Process to establish an ad hoc scientific panel
ECDC has the possibility to establish ad hoc scientific panels that will aid ECDC and provide independent advice on
a topic during a limited time and with a specific scope. The process to set up such an ad hoc scientific panel
follows a strict methodology and includes the following main steps: Identification of experts; collecting declarations
of interests of experts; evaluating the eligibility and rule out conflict of interests of experts through clearance by
the ECDC compliance officer; formal appointment of panel members by the ECDC Director.
The identification of experts can be done in several ways: inventory of key experts that publish scientific literature
in the area, request for suggestions of experts by the ECDC Advisory Forum, and through other means that involve
contacting our network and partners for suggestions. It is for ECDC to decide on the composition of the panel,
taking into account for example country/setting representativeness, and balance of specific expertise and
experience of panel members.
Observers
The scientific panel will also be complemented with observers from key stakeholders, such as the European
Commission, WHO Regional Office of Europe, the International Organisation for Migration and representatives from
EU Commission-funded projects. The role of the observers will be to provide scientific advice prior to, during and
after the scientific panel meeting. However, the final formulation of the statements in the ECDC guidance will be
determined by the officially appointed scientific panel for eventual ECDC approval.
Purpose and role of the scientific panel
The scientific panel will follow the Institute of Medicine Standards for Systematic Reviews and Guidelines (2011) to
ensure a rigorous and transparent scientific process.
• The panel will be responsible for thoroughly reviewing the proposed methodology, subsequent evidence
reviews and the final guidance document.
• A review of the proposed methodology will include an assessment of whether the proposed guideline
development process is consistent with the steps described in methods process.
• The panel will also review the options for interventions based on the scientific evidence.
• A review of the final guidance document will ensure that the approved process has been followed.
• The panel will ensure that the final output contains clear and actionable guidance.
Table A-1. Composition of the ad hoc scientific panel
Name
Country
Affiliation
Angel Kunchev
Bulgaria
Ministry of Health, Chief State Health Inspector
Gabrielle Jones
France
Santé publique France, Epidemiologist
Anna Kuehne
Germany
Robert Koch Institute, Epidemiologist
Agoritsa Baka
Greece
Hellenic Centre for Disease Control and Prevention (KEELPNO),
Office for Scientific Advice
Apostolos Veizis
Greece
MSF, Director Medical Operational Support Unit

SCIENTIFIC ADVICE Public health guidance on screening and vaccination for infectious diseases in newly arrived migrants
77
Name
Country
Affiliation
Lelia Thornton
Ireland
HSE Health Protection Surveillance Centre, Specialist in Public
Health Medicine
Silvia Declich
Italy
Istituto Superiore di Sanità (ISS), National Centre for Global
Health, senior epidemiologist
Francesco Castelli
Italy
University of Brescia, Professor
Pierluigi Lopalco
Italy
University of Pisa, Full Professor of Hygiene and Preventive
Medicine
Machiel Vonk
Netherlands
RIVM/LCI, Public health doctor
Maria Van Den Muijsenbergh
Netherlands
Pharos/Radboud University Medical centre Nijmegen, senior
researcher and general practitioner
Sonia Dias
Portugal
National School of Public Health, Universidade Nova de Lisboa,
Professor of Public Health
Henrique Dias Pinto De Barros
Portugal
University of Porto, MD, PHD
Manuel Carballo
Spain
Executive Director, ICMHD
Maria Axelsson
Sweden
Public Health Agency of Sweden, epidemiologist
Dominik Zenner
United Kingdom
Public Health England, Head of TB screening
Ines Campos-Matos
United Kingdom
Public Health England, Consultant Epidemiologist, acting head
of Travel and Migrant Health section
Manish Pareek
United Kingdom
University of Leicester, Department of Infection and HIV
Medicine, DR
Rebecca Hall
United Kingdom
Mawbey Group Practice Darzi Fellow, North West London
Collaboration of CCGs Clinical Support Fellow, RCGP, GP

ECDC is committed to ensuring the transparency and independence of its work
In accordance with the Staff Regulations for Officials and Conditions of Employment of Other Servants of the European Union and the
ECDC Independence Policy, ECDC staff members shall not, in the performance of their duties, deal with a matter in which, directly or
indirectly, they have any personal interest such as to impair their independence. Declarations of interest must be received from any
prospective contractor(s) before any contract can be awarded.
www.ecdc.europa.eu/en/aboutus/transparency
HOW TO OBTAIN EU PUBLICATIONS
Free publications:
• onecopy:
viaEUBookshop(http://bookshop.europa.eu);
• morethanonecopyorposters/maps:
fromtheEuropeanUnion’srepresentations(http://ec.europa.eu/represent_en.htm);
fromthedelegationsinnon-EUcountries(http://eeas.europa.eu/delegations/index_en.htm);
bycontactingtheEuropeDirectservice(http://europa.eu/europedirect/index_en.htm)or
calling 00 800 6 7 8 9 10 11 (freephone number from anywhere in the EU) (*).
(*)Theinformationgivenisfree,asaremostcalls(thoughsomeoperators,phoneboxesorhotelsmaychargeyou).
Priced publications:
• viaEUBookshop(http://bookshop.europa.eu).
European Centre for Disease
Prevention and Control (ECDC)
Address:
GustavIII:sboulevard40,SE-16973Solna,
Sweden
Tel.+46858601000
Fax+46858601001
www.ecdc.europa.eu
An agency of the European Union
www.europa.eu
Subscribe to our publications
www.ecdc.europa.eu/en/publications
Contact us
publications@ecdc.europa.eu
Follow us on Twitter
@ECDC_EU
Like our Facebook page
www.facebook.com/ECDC.EU

{kind=link}