
February 2008
ProcessCover.ai 3/5/2008 10:11:38 AM

Suggested Citation
Centers for Disease Control and Prevention. Introduction to Process Evaluation in Tobacco Use Prevention and
Control. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention,
National Center for Chronic Disease Prevention and Health Promotion, Oce on Smoking and Health; 2008.
Available at: http://www.cdc.gov/tobacco/publications/index.htm.
Introduction to Process
Evaluation in Tobacco Use
Prevention and Control
February 2008

ACKNOWLEDGEMENTS
The manual was prepared by the Centers for Disease Control and Prevention, Oce on Smoking and Health.
Matthew McKenna, Director
Corinne Husten, Branch Chief, Epidemiology Branch
Robert Merritt, Team Lead, Evaluation Team
Donald Compton, Project Lead
Nicole Kuiper
Sheila Porter
Contributing Authors
Paul Mattessich, Wilder Research Center
Patricia Rieker, Boston University
Battelle Centers for Public Health Research and Evaluation
Pamela Clark
Mary Kay Dugan, Task Leader
Carol Schmitt
RTI International
Barri Burrus
Suzanne Dolina
Erika Fulmer, Task Leader
Maria Girlando
Michelle Myers
We thank the members of the Editorial Review Group and the Expert Panel for contributing their expertise and
experience in developing and reviewing this manual.
Editorial Review Group
Centers for Disease Control and Prevention
Deborah Borbely
Robert Merritt
Michael Schooley
Gabrielle Starr
Debra Torres
Tobacco Technical Assistance Consortium
Pamela Redmon
State Health Department Representatives
Jennifer Ellsworth, Minnesota
Lois Keithly, Massachusetts
Mike Placona, North Carolina
Scott Proescholdbell, North Carolina
Saint Louis University
Douglas Luke
Nancy Mueller
i

Expert Panel
Centers for Disease Control and Prevention
Deborah Borbely
Robert Robinson
Michael Schooley
Brick Lancaster
Patty McLean
Lisa Petersen
Gabrielle Star
Deborah Torres
Michael Baizerman, University of Minnesota
Ursula Bauer, New York Department of Health
Robert Goodman, University of Pittsburgh
Donna Grande, American Medical Association
Paul Mattessich, Wilder Research Center
Edmund Ricci, University of Pittsburgh
Todd Rogers, Public Health Institute
Stacy Scheel, More Voices, Inc.
Laura Linnan, University of North Carolina
Douglas Luke, Saint Louis University
Karla Sneegas, Indiana Tobacco Prevention and Cessation Agency
Frances Stillman, Johns Hopkins University
CDC acknowledges the following National Tobacco Control Program (NTCP) program managers and their sta for
participating in interviews to identify key factors associated with successful tobacco use prevention and control
programs. We also thank the Ohio Tobacco Use Prevention and Control Foundation for their participation.
Joann Wellman Benson, California
Karen DeLeeuw, Colorado
Joan Stine, Maryland
Lois Keithly, Massachusetts
Paul Martinez, Minnesota
Sally Malek, North Carolina
Terry Reid, Washington
Joan Stine, Ohio
Ken Slenkovitch, Ohio Tobacco Use Prevention and Control Foundation
ii

Contents
Contents
Section Page
Acknowledgements i
1. Introduction 1
1.1 The Planning/Program Evaluation/Program Improvement Cycle...................................................................... 2
1.2 Distinguishing Process Evaluation from Outcome Evaluation ............................................................................ 3
2. Purposes and Benets of Process Evaluation 4
2.1 Denition of Process Evaluation..................................................................................................................................... 4
2.2 Scope of Tobacco Control Activities Included in a Process Evaluation............................................................. 4
2.3 Purposes: How Does Process Evaluation Serve You?............................................................................................... 4
2.3.1 Program Monitoring .......................................................................................................................................... 5
2.3.2 Program Improvement ..................................................................................................................................... 5
2.3.3 Building Eective Program Models..............................................................................................................7
2.3.4 Accountability...................................................................................................................................................... 7
2.4 Users and Uses of Process Evaluation Information ................................................................................................11
2.4.1 Users ......................................................................................................................................................................11
2.4.2 Uses........................................................................................................................................................................14
3. Information Elements Central to Process Evaluation 17
3.1 Indicators of Inputs/Activities/Outputs .....................................................................................................................17
3.2 Comparing Process Information to Performance Criteria ...................................................................................21
4. Managing Process Evaluation 29
4.1 Managing Process Evaluation: A 10-Step Process ..................................................................................................29
4.1.1 Purpose: Why Use the 10-Step Process for Managing Evaluation?.................................................29
4.1.2 Roles of the Advisory Group, Evaluation Facilitator, and Evaluator................................................30
4.1.3 Stages and Steps of the 10-Step Process .................................................................................................31
4.1.4 Lessons Learned From Implementing the 10-Step Process ..............................................................35
4.2 The Program Evaluation Standards and Protecting Participants in Evaluation Research........................37
4.2.1 The Program Evaluation Standards...................................................................................................................37
iii

Contents
4.2.2 Protecting Participants in Evaluation Research ............................................................................................38
4.3 Choosing a Process Evaluation Design (Methodology) .......................................................................................39
4.4 Process Evaluation—Beyond a Single Study............................................................................................................41
5. Conclusion 43
Glossary of Terms 45
Appendices
A CDC’s Framework for Program Evaluation ................................................................................................................47
B Detailed List ofThe Joint Committee on Standards for Evaluation: The Program Evaluation Standards...49
C Additional Information on the Purpose, Selection, and Roles of the Evaluation Advisory Group .......53
D Process Evaluation Questions and Logic Model from the Center for Tobacco Policy Research ............57
References 59
iv

Exhibits
EXHIBITS
Number Page
1-1 CDC’s Framework for Program Evaluation ........................................................................................................................... 2
1-2 Logic Models................................................................................................................................................................................... 3
2-1 Four Primary Purposes of Process Evaluation ..................................................................................................................... 8
3-1 Information Commonly Obtained in a Process Evaluation ..........................................................................................18
3-2 Inputs—Comparing Indicators to Criteria..........................................................................................................................22
3-3 Activities and Outputs—Comparing Indicators to Criteria..........................................................................................24
3-4 Tobacco-Related Disparities: Activities and Outputs—Comparing Indicators to Criteria................................25
4-1 Overview of the 10-Step Process for Managing Evaluation.........................................................................................32
4-2 Steps and Sta Responsibilities in the 10-Step Process ................................................................................................33
D-1 Strategy 1 Logic Model: Show Me Health—Clearing the Air About Tobacco .......................................................58
Case Examples Based on Logic Model Categories
Assessment of Learning from truth
sm
: Youth Participation in Field Marketing Techniques to Counter Tobacco
Advertising ...................................................................................................................................................................................... 9
Outcome and Process Evaluation of a School-Based, Informal, Adolescent Peer-Led Intervention to Reduce
Smoking..........................................................................................................................................................................................10
Stakeholder Advisory Board: The North Carolina Youth Empowerment Study.....................................................................13
Assessing the Eectiveness of a Training Curriculum for Promotores, Spanish-Speaking Community Health
Outreach Workers........................................................................................................................................................................14
Assessment of Use of Best Practices Guidelines by 10 State Tobacco Control Programs ..................................................15
Incorporating Process Evaluation Findings into Development of a Web-Based Smoking Cessation Program for
College-Aged Smokers..............................................................................................................................................................16
Case Examples Based on Process Information Components
Implementation of the Henry J. Kaiser Family Foundation’s Community Health Promotion Grant Program............26
New York Statewide School Tobacco Policy Review........................................................................................................................27
Elimination of Secondhand Smoke through the Seattle and King County Smoke-Free Housing Initiative ...............28
v

Introduction
1. INTRODUCTION
Tobacco use in the United States is the single most preventable cause of death and disease.
1
The Centers for
Disease Control and Prevention’s Oce on Smoking and Health (CDC/OSH) created the National Tobacco Control
Program (NTCP) to foster and support coordinated, nationwide, state-based activities to advance its mission to
reduce disease, disability, and death related to tobacco use.
CDC/OSH has identied four program goal areas:
• Preventing initiation of tobacco use among young people;
• Eliminating nonsmokers’ exposure to secondhand smoke;
• Promoting quitting among adults and young people; and
• Identifying and eliminating tobacco-related disparities.
To determine the eectiveness of NTCP programs, both their implementation and their outcomes must be
measured.
2
This manual is intended to provide process evaluation technical assistance to OSH sta, grantees and partners. It
denes process evaluation and describes the rationale, benets, key data collection components, and program
evaluation management procedures. It also discusses how process evaluation links with outcome evaluation and
ts within an overall approach to evaluating comprehensive tobacco control programs. Previous CDC initiatives
have provided resources for designing outcome evaluations. (See, for example, the CDC framework depicted in
Exhibit 1-1.) This manual complements CDC’s approach to outcome evaluation by focusing on process evaluation
as a way to document and measure implementation of NTCP programs.
The content of this manual reects the priorities of CDC/OSH for program monitoring and evaluation, and
augments two other CDC/OSH publications: Key Outcome Indicators for Evaluating Comprehensive Tobacco Control
Programs
3
and Introduction to Program Evaluation for Comprehensive Tobacco Control Programs.
2
This manual:
• Provides a framework for understanding the links between inputs, activities, and outputs and for assessing
how these relate to outcomes; and
• Can assist state and federal program managers and evaluation sta with the design and implementation
of process evaluations that will provide valid, reliable evidence of progress achieved through their tobacco
control eorts.
As you read this manual, keep in mind that it is not a “cookbook” for process evaluation. State and local programs
have unique features and contexts that create a need for dierent types of process-related information. This
manual does explain general principles of process evaluation and provides a guide for determining what
types of information to gather. Also, be mindful that process evaluation of an overall comprehensive state
program such as tobacco control is not typically conducted because the scope of such an evaluation would
1

Introduction to Process Evaluation in Tobacco Use Prevention and Control
not be practical and would be extremely costly. Rather, process evaluation is typically used to evaluate a given
component or activity within an overall comprehensive program. Finally, please note that for the purposes of
this manual, the terms program, project, and intervention are used interchangeably.
1.1 The Planning/Program Evaluation/Program Improvement Cycle
Evaluation is a systematic process to understand what a program does and how well the program does it.
Evaluation results can be used to maintain or improve program quality and to ensure that future planning can
be more evidence-based. Evaluation constitutes part of an ongoing cycle of program planning, implementation,
and improvement.
Exhibit 1-1 provides a visual representation of the six-step CDC framework for general program evaluation.
4
The six steps in the CDC framework represent an ongoing cycle, rather than a linear sequence, and addressing
each of the steps is an iterative process.
4
Implicit in the framework is the connection between evaluation and
planning. Additional information about each step is provided in Appendix A.
Exhibit 1-1: CDC’s Framework for Program Evaluation
Standards
Utility
Feasibility
Propriety
Accuracy
Steps
1. Engage
Stakeholders
2. Describe
the Program
3. Focus the
Evaluation Plan
4. Gather Credible
Evidence and
Support
5. Justify
Conclusions and
Recommendations
6. Ensure Use
and Share
Lessons Learned
SOURCE: Centers for Disease Control and Prevention. Framework for program evaluation in public health. MMWR
1999;48(RR11):1–40.
2

Section 1—Introduction
1.2 Distinguishing Process Evaluation from Outcome Evaluation
The NTCP is guided by logic models which address each of the four goals described earlier. The CDC/OSH
approach to tobacco control evaluation is also based in the use of logic models. As shown in Exhibit 1-2, logic
models specify program inputs, activities, outputs, and outcomes (short-term, intermediate, and long-term).
2,3
(See Glossary for denition of terms.)
Exhibit 1-2: Logic Models
Inputs Activities
Intermediate
Outcomes
Long-term
Outcomes
Outputs
Short-term
Outcome
To date, CDC/OSH has developed an approach that emphasizes the last three boxes in Exhibit 1-2, focusing
on outcomes and providing resources to enable program sta to measure and report them. This is outcome
evaluation.
The NTCP has focused on outcome evaluations for several good reasons. Outcome evaluation allows researchers
to document health and behavioral outcomes and identify linkages between an intervention and quantiable
eects. Also, epidemiologists and other practitioners often have a well-developed evidence base for population-
level intervention outcomes, making it feasible to conduct outcome evaluations.
On the other hand, process evaluation focuses on the rst three boxes of the logic model. It enables you to
describe and assess your program’s activities and to link your progress to outcomes. This is important because
the link between outputs and short-term outcomes remains an empirical question. Unlike outcome evaluations,
process evaluations often use practice wisdom (that is, the observations and opinions of professionals in the
eld) to help identify the links between inputs/activities/outputs and short-term outcomes.
A variety of evidence-based guidance is available for NTCP grantees. For example, anticipating the new funds
available to states from the 1998 Master Settlement Agreement (MSA), in 1999, CDC/OSH published Best
Practices for Comprehensive Tobacco Control Programs (Best Practices).
1
This was the rst document to describe the
nine core components of a comprehensive tobacco control program. Best Practices also contained a formalized
set of funding recommendations which helped shape state tobacco control programs by providing national
frameworks and standards.
5
Since Best Practices was released, new guides and reviews have been published. For
instance, the Guide to Community Preventive Services,
6
and the California Communities of Excellence in Tobacco
Control
7
establish planning frameworks that help to dene state activities, expected outputs, and standards
useful for process evaluation. We have included an example of an actual logic model for a process evaluation
(Appendix D), which was provided by the Center for Tobacco Policy Research (CTPR), Saint Louis University
School of Public Health.
3

Introduction to Process Evaluation in Tobacco Use Prevention and Control
2. PURPOSES AND BENEFITS OF PROCESS EVALUATION
This chapter is intended to answer fundamental questions about the value and implementation of process
evaluation within tobacco use prevention and control eorts.
2.1 Denition of Process Evaluation
Process evaluation, as one aspect of overall program evaluation, is:
The systematic collection of information on a program’s inputs, activities, and outputs, as well as the
program’s context and other key characteristics.
Process evaluation involves the collection of information to describe what a program includes and how it
functions over time. In and of itself, the information is “neutral.” It is merely descriptive, although people often
attach meaning and value to the information. It does not reect “quality” until you compare it to an external set
of standards or criteria.
Process evaluations can occur just once, periodically throughout the duration of a program, or continuously. The
type of information gathered, and its frequency, will depend on the kinds of questions that you seek to answer.
2.2 Scope of Tobacco Control Activities Included in a Process Evaluation
In evaluations of tobacco-control programs, a question commonly arises: On what “level of program(s) or
activities” should the evaluation focus? The answer is: The number and type of programs and activities included
in a process evaluation will depend on the interests and questions of stakeholders and the intended uses of the
information.
For example, if the objective of a process evaluation is solely to assess the eorts of a particular program (e.g.,
eorts to increase the cigarette tax or increase use of a quitline), and to improve that program, then a process
evaluation will gather information related only to that program. On the other hand, if the purpose of a process
evaluation is to assess comprehensive tobacco control eorts within a community, a state, or some other
geographic region, then a process evaluation will gather information related to all of the varied programs in
the specied geographic area. As another example, a number of states have already passed smoke-free work
place laws; thus the objective of a process evaluation might be to assess the education, training, and technical
assistance provided to interpret and implement these laws.
2.3 Purposes: How Does Process Evaluation Serve You?
Process evaluation has four primary purposes related to individual programs and to the general eld of
tobacco control: program monitoring, program improvement, development of eective program models, and
accountability. This section provides a brief overview of these purposes, along with case examples. Later in this
manual, you will nd more examples, as well as details on the information you can collect to fulll these purposes.
4

Section 2—Purposes and Benets of Process Evaluation
2.3.1 Program Monitoring
Program monitoring includes tracking, documenting, and summarizing the inputs, activities, and outputs of your
program. So, for example, you may record at one or more points in time:
• How much money is spent,
• The number of sta and/or volunteers involved in the activities of the program,
• The amount and types of activities related to tobacco use prevention and control,
• The number or proportion of people reached,
• The economic, social, and demographic characteristics of people reached, and
• The number of meetings or training sessions conducted.
Second, program monitoring includes the description of characteristics of the program and its context, which
might be important for understanding how and why it worked the way it did. For example, you might note:
• The locale where a program carries out its activities (e.g., rural, urban),
• Demographic or economic characteristics of the target population of the program,
• Amount of training that sta received,
• Age of the program at the time of the evaluation, and
• Unique events that occurred during the course of a program’s eorts.
Careful, reliable monitoring of the inputs, activities, and outputs of your program—along with a description of
the program’s characteristics and context—provides the basic, elemental data necessary for process evaluation.
Such information enables you to determine what you are doing; you can use this information on its own, and
you can use it in connection with the other three purposes of process evaluation or link it with outcomes.
Later, we discuss specic data that process evaluations usually collect for program monitoring. Note, however,
that no hard and fast rules apply to the selection of data to collect. The information that you need will depend on
the questions you want to answer.
2.3.2 Program Improvement
Once you have information about inputs, activities, and outputs, along with information on the characteristics
and context of a program, you can use this information to support decisions regarding program improvement or
future planning.
Consider the example of a quitline program. For those individuals who actually make contact and complete
the program, it may be achieving good quit rates. However, suppose the program suers from insucient
recruitment and retention of participants. Process evaluation can reveal why participation levels fall short
of program objectives. For instance, results may show that the program has some inconvenient features,
5

Introduction to Process Evaluation in Tobacco Use Prevention and Control
lacks optimal language or cultural attributes, or has other characteristics that create barriers. You and your
fellow program managers can then use these ndings to improve the quitline by increasing participation and
completion.
In using process evaluation for program improvement, you will most commonly approach your task in either or
both of two ways:
a. Comparing a program to a standard or expectation (e.g., program goals/objectives, funding
recommendations and guidelines, or standards of practice).
You can compare any of the data that you obtain in a process evaluation to the specic goals or objectives
of your program. For example, you may have targets regarding the number or type of people you will reach
or the amount of service that you will provide. Process evaluation will show whether you are meeting those
targets; if not, you can adjust your eorts accordingly.
Process information (e.g., information on the types of persons reached by the program, languages spoken,
features of the program) can help you understand whether you are reaching specic populations. Process
information can also support your decision-making regarding the best ways to adapt or ne tune the
program to appeal to the broadest array of persons in the intended population.
“Evidence-based” or “best practice” standards
1,6
sometimes exist for a program. When they do, you can
compare your performance to these standards, using process evaluation information. (This is sometimes
called assessing “delity” to established practice standards.) If you discover a lack of alignment with
established standards or guidelines, you can adjust your program for a better t. In the absence of standards
derived from evidence-based research, normative standards can be developed based on the experience of
programs of a similar type. For example, if you are planning a print media campaign, you may learn from
other programs that multi-media campaigns are more eective than print media alone.
b. Relating process data to outcome data.
Program outcome data enable you to know whether you are producing the desired eects. You can examine
your outcome evaluation data and process evaluation data together to identify steps you can take to
increase eectiveness.
In fact, process evaluation is most eective when implemented in conjunction with outcome evaluation.
Knowing what actually occurred as the program was implemented helps you to understand and analyze the
conditions that are responsible for a given outcome. Ideally, process evaluation will allow you to attribute
strengths and/or weaknesses of your program to specic program characteristics or activities. Without this
information, you may nd it very dicult to take action when attempting to improve the program using
only outcome information.
8
6

Section 2—Purposes and Benets of Process Evaluation
2.3.3 Building Eective Program Models
The experiences of multiple programs have shown that the tobacco control eld can use process and outcome
information jointly to build eective program models. Evaluation research can identify, for example, which
activities tend to lead to the best outcomes. This use of process evaluation typically lies outside the purview
of a single program, unless that program is large enough to vary its activities systematically and test how that
variation aects outcomes. More commonly, individual programs will simply report their process and outcome
data to CDC/OSH or in annual reports; or they might participate in a controlled or natural eld experiment.
Controlled scientic experiments to validate evidence-based practices can incorporate process evaluation for
multiple functions. For example, documentation of inputs and activities produces information for comparing
the extent to which experimental and control programs have carried out their work in conformity with
study protocols. Accurate recording of outputs enables researchers to compare the relative productivity of
experimental and control programs. Documentation of activities, as well as unique occurrences that aected
a specic program, can assist in the interpretation of experimental data, in the explanation of anomalies, and
in decisions concerning validity of specic cases to be included in the analysis of an experiment’s ndings. See
also Steckler and Linnan (2002)
9
for a discussion of process evaluation in the development of theory-based
interventions.
2.3.4 Accountability
Process evaluation assists a program in being accountable to its funders, regulators, and other stakeholders,
including government ocials and policy makers. It does so, rst of all, by providing the data necessary to justify
expenditures of time and money—for example, demonstrating the number of materials produced, the amount
of public advertising, the number of people reached or served, and so forth. A clear demonstration of the links
between program inputs, activities, and outcomes enhances justication for funding.
Second, process evaluation supports accountability by documenting compliance with externally imposed
standards
1
or criteria established by program funders for continued funding of the program. For example,
process evaluation can indicate whether stang for a program meets the level recommended by CDC.
See Exhibit 2-1 for more information on the purposes of process evaluation and examples of questions that
process evaluation enables you to answer.
1
These standards are often based on research that has established evidence-based practice, but not necessarily.
7

Introduction to Process Evaluation in Tobacco Use Prevention and Control
Exhibit 2-1: Four Primary Purposes of Process Evaluation
What You Can Do with Process
Evaluation Purpose Sample Questions
1. Program
monitoring
Track, document, and summarize the
inputs, activities, and outputs of a
program.
Describe other relevant characteristics
of the program and/or its context.
• How much money do we spend on this
program?
• What activities are taking place?
• Who is conducting the activities?
• How many people do we reach?
• What types of people do we reach?
• How much eort (e.g., meetings, media
volume, etc.) did we put into a program or
specic intervention that we completed?
2. Program
improvement
Compare the inputs, activities, and
outputs of your program to standards
or criteria, your expectations/plans, or
recommended practice (delity).
Relate information on program inputs,
activities, and outputs to information
on program outcomes.
• Do we have the right mix of activities?
• Are we reaching the intended targets?
• Are the right people involved as partners,
participants, and providers?
• Do the sta/volunteers have the necessary
skills?
3. Building
eective
program models
Assess how process is linked to
outcomes to identify the most
eective program models and
components.
• What are the strengths and weaknesses
within discrete components of a multi-
level program?
• What is the optimal path for achieving a
specic result (e.g., getting smoke-free
regulations passed)?
4. Program
accountability
Demonstrate to funders and other
decision makers that you are making
the best possible use of program
resources.
• Have the program inputs or resources
been allocated or mobilized eciently?
In the following case examples, tobacco control professionals have found process evaluation useful for assisting
with practical issues they face in implemen
ting high quality programs. (Note that these case examples, as well as
the others later in this manual, are tied to specic parts of a logic model and/or to the categories of information
typically gathered in a process evaluation. This link to the model is intended to strengthen the use of process
evaluation within the overall CDC approach to evaluation.)
8

Section 2—Purposes and Benets of Process Evaluation
CASE EXAMPLE BASED ON LOGIC MODEL CATEGORY: ACTIVITIES
Assessment of Learning from truth
®
: Youth Participation in Field Marketing Techniques to Counter
Tobacco Advertising
The truth
®
campaign, a mass-media (print and television) counter-marketing activity targeting youth age
12-17, was funded by the American Legacy Foundation and included a national eld marketing component
(the truth
®
tour). This unique campaign promotes an “edgy youth” brand and provides information about
tobacco, the tobacco industry, and the social costs of tobacco use. It advocates that teens take control of
their lives and reject the inuence of the industry’s advertising practices.The goal is to reach non-mainstream
teens, a group that evidence shows to be at risk for smoking initiation, by using youth who reect the target
audience to sta a eld marketing endeavor.”
How process evaluation was helpful:
The tour was designed to encourage direct youth-to-youth contact to facilitate the transmission of
tobacco counter-marketing information. This unique approach posed several problems for a traditional
outcome evaluation design. The age of the target audience precluded follow-up interviews without
parental permission, so an ethnographic approach was used to provide process evaluation data instead.
Methods consisted of observation, participant-observation, informal conversations, and semistructured and
unstructured open-ended interviews with the tour riders, sta, and adults from the visited communities.
The purpose of the evaluation was program improvement. Data were needed to document tour activities and
group dynamics, and to assess the impact of tour participation on the riders. Riders consisted of three groups
of between 6 and 12 carefully selected, diverse, and specially trained youth (under the age of 18) who visited
27 cities in 2000. The tour created three small, close-knit mobile communities who lived and worked together
for a 6-week period. The tour was built around high visibility trucks painted with the truth
®
logo and specic
music geared to appeal to the targeted audience in selected venues. To avoid undermining the edgy youth
image, no one from the local markets was involved in the planning or implementation of tour activities.
Advantages for you:
The evaluation provided an opportunity to assess the implementation of a unique eld marketing approach
to reaching teens with a public health message about tobacco use. Evaluation results highlight various
lessons learned. The evaluation provided an in-depth understanding of the range and type of diculties
associated with underage, “edgy” culturally diverse riders. A possible alternative would be to hire young
adults who do not need to be supervised as closely while on the road and to involve youth from local markets
in the planning and implementation of the activity. The latter would address the problems that occurred
with visiting venues where none of the target audience appeared. Sensitivity training around issues of race,
ethnicity, sexual preference, and youth culture is required for all adult sta when traveling on the road with
diverse youth. Evaluation results also suggest that eld marketing techniques for a national social marketing
campaign can benet from involvement of a local distribution system for the product or message, in order to
create linkages that might sustain brand visibility and product availability in the community. Closer ties with
local level tobacco control allies who reect the image of the campaign would be a more eective strategy.
SOURCE: Eisenberg M, Ringwalt C, Driscoll D, Vallee M, Gullette G. Learning from truth®: Youth
participation in eld marketing techniques to counter tobacco advertising. Journal of Health
Communication 2004; 9:223-231.
(Continued)
9

Introduction to Process Evaluation in Tobacco Use Prevention and Control
CASE EXAMPLE BASED ON LOGIC MODEL CATEGORY: ACTIVITIES and OUTPUTS
Outcome and Process Evaluation of a School-Based, Informal, Adolescent Peer-Led Intervention to
Reduce Smoking
Peer education as a strategy for youth health promotion is used extensively, although there is mixed evidence
for its eectiveness. There are few systematic accounts of what young people actually do as peer educators. To
examine the activities of the young people recruited as “peer supporters” for A Stop Smoking in Schools Trial
(ASSIST) in southeast Wales and the West of England, 10,730 students in 59 secondary schools were recruited
at baseline. The ASSIST peer nomination procedure was successful in recruiting, training, and retaining
inuential year 8 peer supporters of both genders to intervene informally to reduce smoking levels in their
year group.
How process evaluation was helpful:
Outcome data at 1-year follow-up showed that the risk of students who were occasional or experimental
smokers at baseline reporting weekly smoking at follow-up was 18.2% lower in the intervention schools.
This result was supported by analysis of salivary cotinine. To understand how this short-term outcome was
achieved, researchers assessed qualitative data from the process evaluation. These data showed that the
majority of peer supporters adopted a pragmatic strategy: they concentrated their attention on friends and
peers who were occasional or non-smokers and whom they felt could be persuaded not to take up smoking
regularly, rather than those they considered to be already “addicted” or who were members of smoking
cliques.
Advantages for you:
By combining process and outcome evaluation, the authors were able to identify how the peer supporters
actually implemented the intervention to achieve the outcome. The study showed that school-based peer
educators are eective in diusing health promotion messages when they are asked to work informally
rather than under the structured supervision of teaching sta. The smoking behavior of the peer supporters
themselves also appears to have been aected by the training. Though not encouraged to use fear-based
approaches (as best practice would suggest) the peer educators actually employed such tactics eectively.
While the message delivered by the peer educators was relatively unsophisticated and soon appeared to lose
momentum, a two-year follow-up will substantiate whether the reduction in smoking levels is maintained.
SOURCE: Audrey A, Holliday J, Campbell R. It’s good to talk: Adolescent perspectives of an informal,
peer-led intervention to reduce smoking. Social Science and Medicine 2006;63:320-334.
10

Section 2—Purposes and Benets of Process Evaluation
2.4 Users and Uses of Process Evaluation Information
2.4.1 Users
There are three major groups of stakeholders integral to program evaluation:
• Those served or aected by the program, such as patients or clients, advocacy groups, community members,
and elected ocials;
• Those involved in program operations, such as management, program sta, partners, the funding agency or
agencies, and coalition members; and
• Those in a position to make decisions about the program, such as partners, the funding agency, coalition
members, and the general public.
A primary feature of an eective evaluation is the identication of the intended users who can most directly
benet from an evaluation.
8
A rst step should be to identify evaluation stakeholders, including those who
have a stake or vested interest in evaluation results, as well as those who have a direct or indirect interest in
program eectiveness.
8
Identication and engagement of intended users in the evaluation process will help
increase use of evaluation information. These intended users are more likely to understand and feel ownership
in the evaluation process if they have been actively involved in it.
8
Additionally, such engagement enhances
understanding and acceptance of the utility of evaluation information throughout the lifecycle of a program. So,
to ensure that information collected, analyzed, and reported successfully meets the needs of stakeholders, you
should work with the people who will be using this information from the beginning of the evaluation process
and focus on how they will use it to answer what kind of questions.
The following are possible stakeholders in tobacco prevention and control programs:
• Program managers and sta
• Local, state, and regional coalitions interested in reducing tobacco use
• Local recipients of tobacco-related funds
• Local and national partners (such as the American Cancer Society, the American Lung Association,
the American Heart Association, the Centers for Disease Control and Prevention, the American Legacy
Foundation, the Substance Abuse and Mental Health Services Administration, and the Robert Wood Johnson
Foundation)
• Funding agencies, such as national and state governments or foundations
• State or local health departments and health commissioners
• State education agencies, schools, and educational groups
• Universities and educational institutions
• Local government, state legislators, and state governors
11

Introduction to Process Evaluation in Tobacco Use Prevention and Control
• Privately owned businesses and business associations
• Health care systems and the medical community
• Religious organizations
• Community organizations
• Private citizens
• Program critics
• Representatives of populations disproportionately aected by tobacco use
• Law enforcement representatives
As you review this list, consider that many of these stakeholders have diverse and, at times, competing
interests. Given that a single evaluation cannot answer all possible issues raised by these diverse interests,
the list of stakeholders must be narrowed to a more specic group of primary intended evaluation users; the
recommended number of primary intended evaluation users is 8-10.
10
These stakeholders/primary intended
users will serve in advisory roles on all phases of the evaluation, beginning with identication of primary
intended uses of the evaluation (see Section 4).
To identify the primary intended users, you and your program collaborators should identify all possible
stakeholders and determine how critical it is for the ndings of the evaluation to inuence each stakeholder.
Only those stakeholders whom you want to be inuenced and to take action (as opposed to those for whom
information is valuable to know, but not critical) should be included as primary intended users.
12

Section 2—Purposes and Benets of Process Evaluation
CASE EXAMPLE BASED ON LOGIC MODEL CATEGORY: INPUTS
Stakeholder Advisory Board
The North Carolina Youth Empowerment Study
The North Carolina Youth Empowerment Study (NC YES) was a three-year participatory evaluation of youth-
based tobacco use prevention programs. The study aimed to document the characteristics of youth tobacco
use and prevention programs throughout North Carolina, and to track the role youth in these programs
played in implementing tobacco-free policies within local school districts.
How process evaluation was helpful:
One important component of the project involved convening an advisory board of key program stakeholders,
including both youth and adults. The purpose of the advisory board was to provide input on all aspects of
the study, including the study’s research questions, data collection strategies, and interpretation of results.
Board members were selected to reect the racial, ethnic, and geographic diversity of the state, as well as the
diversity within types of participating organizations.
Advantages for you:
The benets of this collaboration were apparent to both researchers and stakeholders who were members of
the advisory board. For example, the research team was able to use the board’s input on the data collection
tools so that the information collected would be of greater use to the community. The board also requested
that the research team disseminate results beyond the university so that a wider audience would have access
to the ndings. Being involved in the process beneted board members through increased knowledge of
evaluation and research methods. They also felt that their experiences and skills had been utilized through
the participatory process and that the information disseminated beneted multiple audiences, not just the
research community.
SOURCE: Ribisl KM, Steckler A, Linnan L, Patterson CC, Pevzner E, Markatos E, et al. The North Carolina
Youth Empowerment Study (NC YES): A participatory research study examining the impact of
youth empowerment for tobacco use prevention. Health Education & Behavior 2004;31(5):597–614.
13

Introduction to Process Evaluation in Tobacco Use Prevention and Control
CASE EXAMPLE BASED ON LOGIC MODEL CATEGORY: ACTIVITIES
Assessing the Eectiveness of a Training Curriculum for Promotores, Spanish-Speaking Community
Health Outreach Workers
Tobacco Free El Paso’s objective was to recruit and train promotores who would deliver comprehensive
tobacco cessation interventions (including free nicotine replacement therapies) to low-income,
predominantly Spanish-speaking populations of smokers. Although promotores are used along the U.S.-
Mexico Border to conduct health education classes on topics related to diabetes and other health-related
conditions, there is no research on what role they can play as tobacco cessation counselors.
How process evaluation was helpful:
The training courses (each of which lasted ve days) oered three levels of certication: an introductory basic
skills level; intermediate treatment specialist; and, advanced “leave the addiction” specialist. Over a one-year
period (August 2003–August 2004), 24 training courses involving 89 participants were delivered. Process
information was obtained on the 74 participants who were certied for the introductory level. Of these, 39
went on to the intermediate level and 34 to the advanced certication. To determine the course’s eect on
self-condence and satisfaction, participants were given pre- and post-test measures. While self-condence
improved in all participants, those who completed all the three levels showed the most signicant increase
and were judged capable of delivering a brief smoking cessation intervention. High satisfaction scores
indicated that participants felt adequately prepared.
Program sta used this information to validate the program’s success and to improve implementation of their
“train the trainer” model. The fact that the training courses were easily accessible and free of charge increased
attendance. But the length of the course had a deterrent eect as indicated by the smaller number who
completed the higher levels of training. As a result, the 5-day training session was shortened to 1-, 2-, and
3-day sessions in order increase the number of participants who advance to the higher training levels. This
change was necessary to accommodate participants’ diverse work schedules.
Advantages for you:
Promotores who successfully completed the entire program became part of an extended “train the trainer”
team, with the intention of producing broad population change, and reducing disparities for low-income,
Spanish-speaking people in El Paso. Program sta used the process information to rene the program’s
activities and maximize the number of promotores who would undergo the full training program. Similarly,
you can monitor activities, record participation, and assess satisfaction in order to adjust programs
systematically to eliminate problems that might be reducing your eectiveness.
SOURCE: Martinez-Bristow Z, Sias JJ, Urquidi U, Feng C. Tobacco cessation services through community
health workers for Spanish-speaking populations. American Journal of Public Health, Field Action
Report 2006;96(2): 211-213.
2.4.2
Users
As discussed earlier in this chapter, process evaluations can serve a variety of purposes and can be useful in
dierent ways. Below are two examples of how ongoing process evaluations were used to improve program
guidance and programmatic activities.
14

Section 2—Purposes and Benets of Process Evaluation
CASE EXAMPLE BASED ON LOGIC MODEL CATEGORY: INPUTS
Assessment of Use of Best Practices Guidelines by 10 State Tobacco Control Programs
The Best Practices for Comprehensive Tobacco Control Programs developed by CDC/OSH in 1999 was the rst
national resource to dene the required components of a comprehensive tobacco control program. The
guidelines provide a framework for planning and implementing tobacco control activities. The questions
addressed in the qualitative process evaluation were whether and how states used the guidelines in their
program planning, and what strengths and weaknesses of the guidelines could be identied. During
2002-2003, process evaluation data were collected and analyzed from 10 state tobacco control programs
on familiarity, funding, and use of the guidelines. Information was obtained through written surveys and
qualitative interviews with key tobacco partners in the states. The typical number of participants interviewed
was 17, representing an average of 15 agencies per state.
How process evaluation was helpful:
The results showed that lead agencies and advisory agencies were most familiar with the guidelines, while
other state agencies were less aware of them. Most states modied the guidelines to develop frameworks that
were tailored to their context. For example, many states prioritized the nine components and expenditures
according to their own available resources because funding levels were not always realistic.
Advantages for you:
The results show that the strength of the guidelines included providing a basic framework for program
planning and specic funding recommendations. Limitations included the fact that the guidelines did not
address implementation strategies or tobacco-related disparities, and had not been updated with current
evidence-based research. To ensure that the guidelines continued to be useful to the states, the evaluators
recommended that the guidelines be updated to address implementation of program components,
identify strategies to reduce tobacco-use disparities, and include evidence-based examples. Recommended
funding levels also need to be revised to be more eective in changing social and political climates, and, the
guidelines need to be disseminated beyond typical lead agencies to other tobacco control partners, such as
coalitions and relevant state agencies.
SOURCE: Mueller N, Luke D, Herbers S, Montgomery T. The best practices: Use of the guidelines by ten
state tobacco control programs. American Journal of Preventive Medicine 2006;31(4).
15

Introduction to Process Evaluation in Tobacco Use Prevention and Control
CASE EXAMPLE BASED ON LOGIC MODEL CATEGORY: ACTIVITIES
Incorporating Process Evaluation Findings into Development of a Web-Based Smoking Cessation
Program for College-Aged Smokers
College-aged smokers often do not use traditional cessation methods, such as support groups and
counseling, to reduce their levels of smoking. Therefore, this study aimed to explore the option of an Internet-
based cessation intervention, Kick It!, designed especially for college students. The purpose of the study
was to develop the system and conduct a process evaluation to understand usage and acceptability of the
intervention, as well as to obtain other feedback.
How process evaluation was helpful:
Thirty-ve smokers participated in the intervention, and the research team conducted qualitative interviews
with 6 of the 35 students. The interviews were designed to obtain more information on student use of the
Kick It! program, their thoughts on the program’s strengths and weaknesses, and their recommendations for
future change. The in-depth interviews uncovered several useful suggestions for adding components to the
program, creating a more personalized system, and making format and content changes.
Advantages for you:
The information collected from respondents was detailed enough to allow Kick It! developers to improve
the program for future users and for other researchers to review the work conducted through this process
evaluation to inform development of similar programs for college-aged students.
SOURCE: Escoery C, McCormick L, Bateman K. Development and process evaluation of a Web-based
smoking cessation program for college smokers: Innovative tool for education. Patient Education
and Counseling 2003; 53:217–5.
16

Section 3—Information Elements Central to Process Evaluation
3. INFORMATION ELEMENTS CENTRAL TO PROCESS EVALUATION
3.1 Indicators of Inputs/Activities/Outputs
In a process evaluation, you will collect indicators related to the rst three categories of an evaluation logic
model (inputs, activities, and outputs):
2
• Input indicators measure the various resources that go into a program. Inputs for a tobacco control program
can relate to stang, funds, and other resources.
• Activity indicators measure the actual events that take place as part of a program. In tobacco control, these
events could include youth education campaigns, messages delivered via the media, coalition development,
and many other types of eorts.
• Output indicators measure the direct products of a program’s activities. Examples include the number of
participants using a smoking quitline, a completed media campaign, a higher cigarette tax, the number of
posters placed in stores and buses, and other products.
The following table (Exhibit 3-1) lists typical information elements gathered through process evaluation,
describes them, and provides examples of measures or indicators
2
that can provide this information. The rst
three sets of information elements appear within the categories of inputs, activities, and outputs. Next, some
additional information elements that relate holistically to the overall program and/or its context are listed.
Note that the types of information you collect will depend on the program’s objectives and should be related
to the questions the process evaluation will address. For example, it is typically very important to obtain
information on the characteristics of persons reached or otherwise aected by your program or policy/
regulations. However, which characteristics will you choose to monitor? Gender? Ethnicity? Age? In designing
your process evaluation, the characteristics you select to measure will depend on your specic information
needs. So, for example, if an evidence-based program applies only to a specic age group, you will want
to measure age; or if you need to understand dierences in outcomes among persons of dierent ethnic
backgrounds, then you will want to measure ethnicity.
2
In some cases, a single information element constitutes an indicator on its own (e.g., the number of sta ). In other cases, two
or more elements combine to make a meaningful indicator (e.g., dollars spent per capita).
17

Introduction to Process Evaluation in Tobacco Use Prevention and Control
Exhibit 3-1: Information Commonly Obtained in a Process Evaluation
Item Description Example Process Indicators
1
Inputs
Financial Revenues to support prevention and
control activities, by source; costs
(total or specic to each activity)
Expenses for sta, supplies, media, etc.
Dollars spent per capita
Sources of funds
Personnel—
Quantity
The number of paid sta and/or
volunteers involved;
hours of paid sta and volunteers
Number of sta who carry out the prevention/
control activities
Hours of eort to produce a product
Personnel—
Professional
Characteristics
Qualications/experience/ training of
sta/volunteers involved
Number of sta with special certication
Educational background of sta and
volunteers
Personnel—
Personal
Characteristics
Individual characteristics of sta/
volunteers involved
Ethnic background of sta
Age of sta
Gender of sta
Facilities Key characteristics of the building(s)
and equipment
Hours of operation
Accessibility
Technological capability
Locale Location where the initiative occurs or
the program operates
Geographic scope of prevention/control
activities
Neighborhood type (e.g., urban)
Activities
Population-
oriented
prevention activity
Description of activities to discourage
use or exposure voluntarily, or to
eliminate use or exposure legally—
focused on the community or a
segment of the community
Whether and how counter-marketing occurs
Whether and how information is presented to
legislators
Whether and how technical assistance is
provided to agencies
Individual-
oriented activity
Description of activities directed
toward individuals, on an individual
basis or in dened groups
Type of training
Type of counseling
Accessibility Characteristics of the program that
facilitate exposure to the intervention
Language of campaign materials
Time of day that program is oered
Languages spoken by sta and/or volunteers
Proximity to mass transit
Recruitment Processes for identifying,
approaching, and engaging targeted
audience
Type of contact
Means of advertising
Incentives used to engage audience
18

Section 3—Information Elements Central to Process Evaluation
Exhibit 3-1: Information Commonly Obtained in a Process Evaluation (continued)
Item Description Example Process Indicators
Outputs
Persons reached The number of people with
documented exposure to messages or
who participate in prevention/control
activities
Number of people reached
Number of class participants
Characteristics of
persons reached
Demographic, family, personal,
health, and other attributes of the
people reached by prevention/control
activities
Age
Gender
Comparison of characteristics of persons
reached with characteristics of the intended
target population
Products resulting
from prevention/
control activities
Amount of messages, public
meetings, advertisements,
promotional segments in TV, radio,
newspapers; and, if applicable, service
units delivered
Number of advertisements
Amount of donated air time
Number of meetings with legislators
Number of course sessions
Number of public meetings
Gross Rating Points (GRPs)
Documents that
inuence tobacco
control in a target
area
Written plans, guidelines, or other
documents that inuence the pattern
of tobacco control activities (systems,
partnerships, campaigns, service
delivery) within a target area
Completed state plan
Other Elements Relating to an Initiative/Program as a Whole or to its Context
Developmental
stage
Description of program’s maturity/
current stage of activities
Stage, e.g.:
• Formative/planning
• Early implementation
• Established but still being modied
• Established but stable
• In decline
Organizational
structure and
components
Description of the makeup of the
organization, task force, coalition,
etc., that oversees and implements
program activities, including
accountability for distinct activity
modules, as well as other relevant
structural, leadership, service delivery,
and/or administrative processes
• Name(s) of organization(s) involved,
overall and for each major portion of the
activities
• Aliations of managers
• Type of inter-agency agreement, if any
(Continued)(Continued)
19

Introduction to Process Evaluation in Tobacco Use Prevention and Control
Exhibit 3-1: Information Commonly Obtained in a Process Evaluation (continued)
Item Description Example Process Indicators
Program theory
and delity
Presence or absence of elements/
characteristics of tobacco prevention/
control activities that have been
specied through previous research,
guidelines, and the development of
protocols
• Checklist of steps or guidelines specied
in best practice instructions
• Chronology of signicant implementation
actions
• Identication of events that interfered
with planned activities or implementation
of activities
Collaborations/
partnerships
Extent to which a program involves
multiple independent agencies joined
in a formal arrangement and mutually
accountable for all or part of the work
• Membership lists
• Inter-agency agreements
• Roles of each partner
• Survival of the collaboration for the
duration of the activities
Social, political,
economic
environment
in area of focus
for the tobacco
prevention/
control activities
Elements of the social, political, and
economic conditions that aect the
planning, implementation, and/or
evaluation of the activities intended
to be implemented by a program
• Opinions about tobacco control in
legislature or among the general public
• Major economic trends in area
• Legislation/regulations that enhance
or impede tobacco prevention/control
activities
• Tobacco industry activities and
promotions
Other unique
occurrences
Events within or outside of a program
that aect its implementation or
ongoing operations
• Disruptive social, historical, or
environmental events that inuence
program activities, accessibility, or reach
• Delays in acquisition of nancial
resources, sta, equipment, etc.
20

Section 3—Information Elements Central to Process Evaluation
3.2 Comparing Process Information to Performance Criteria
The specic information elements you collect will depend both on the type of tobacco prevention/control
activities you intend to implement as well as the questions you need to answer through your process evaluation.
As mentioned earlier, process information, in and of itself, is neutral. It does not indicate quality, delity, success,
or compliance. However, you can use process information to assess your progress, provided you establish a
standard or a criterion with which to compare that information.
A standard upon which to compare the process information can be established by using one or more of the
following types of criteria:
• Performance criteria from a funder (e.g., CDC program announcement, foundation RFP);
• Criteria developed as part of the program planning and development process (e.g., SMART objectives,
strategic plan);
• Criteria developed as part of the evaluation planning process (e.g., by an evaluator in consultation with
program sta or a diverse group of stakeholders such as a subgroup of the tobacco control coalition).
Each of these approaches should be supported by scientic guidance of evidence-based programming such
as Best Practices for Comprehensive Tobacco Control Programs,
1
The Guide to Community Preventive Services,
6
and
Communities of Excellence in Tobacco Control.
7
In addition, such criteria should be reasonable within the local
context.
To briey illustrate how process indicators can be compared to hypothetical criteria, we present example inputs,
activities, and outputs that were gathered through eld interviews during full-day site visits with nine states,
discussion groups with state tobacco control sta nationwide, and literature reviews. These are examples of the
inputs, activities, and outputs identied as key elements of comprehensive tobacco use prevention and control
programs.
The comparison of actual inputs, activities, and outputs (as measured through process evaluation) to established
criteria can assist state and territorial tobacco control managers in:
• Identication of discrepancies between planned and actual implementation of the program or intervention;
• Identication of eective and ineective implementation and management strategies; and,
• Improved understanding of whether and how program activities contribute to achieving desired short-term
outcomes.
21

Introduction to Process Evaluation in Tobacco Use Prevention and Control
In Exhibits 3-2, 3-3, and 3-4, we provide examples of how process information can inform decisions about
programmatic issues such as these. It is very important to note that these are merely examples for you to
consider in developing your own criteria and indicators, and they should not be considered as recommended by
CDC for adoption.
Exhibit 3-2 lists example inputs, example criteria for measuring these against, and example indicators for
measuring them.
Exhibit 3-2: Inputs—Comparing Indicators to Criteria
Type of Input Example Criteria
Example Input Indicators
Funding
CDC-r
ec
ommended levels per Best Practices
guidelines
Dollars allocated for each program
component
Stang Required or recommended stang as
described in CDC funding opportunity
announcement (FOA)
Actual stang
Sta Skills 50% of sta will be trained in cultural
competence and 85% will of those trained
will assess the training as high quality
Percentage of sta trained in cultural
competence, and percentage who assess
training as high quality
Partnerships 75% of partners perceive the state as
inclusive of their views in its planning and
implementation
Survey/interview data on partners’
perceptions of the degree to which the
state is inclusive of their views in its
planning and implementation
Specic community or statewide initiatives or programs will select activities that they feel best t the population
they want to address with the nancial resources available, and with respect to political, social, and cultural
considerations. Activities they might select appear in the rst column of Exhibit 3
-3. Please note that these
activities may be carried out by NTCP grantees, partners collaborating with the grantees, or partners on their
own.
For each activity implemented, outputs can also be measured. If output standards exist or are developed, you
can c
ompar
e actual outputs to expected outputs. Example activities with corresponding outputs, including
example criteria and indicators for each, are listed in Exhibit 3-3. While Exhibit 3-1 provides a description of
some of these types of activities, the following criteria contain evaluative components. This ensures that the
information gathered includes not only a description of the activity, but also an assessment of the quality of
that activity. In the rst example (i.e., counter-marketing), the output not only includes the percentage of the
population reached, but also an assessment of the cultural appropriateness of the message.
22

Section 3—Information Elements Central to Process Evaluation
In order to clarify how to understand and use Exhibit 3-3, the following example related to counter-marketing
is provided.
A state health department conducted an evaluation survey and found that compared to other
groups, African-Americans were less likely to report having smoke-free home and automobile
rules, and their children were more likely to be exposed to secondhand smoke. To address
these disparities, the tobacco foundation in the state provided a grant to conduct a multi-
channel counter-marketing campaign to inuence knowledge, attitudes, and behaviors of
African-Americans related to secondhand smoke exposure. Results of a process evaluation
of the counter-marketing campaign showed that it was implemented in print and radio,
and TV via public service announcements (PSAs) rather than paid spots. When planning the
campaign, the state established the criteria that 75% of African-American adults will recall
the campaign messages and perceive them to be appropriate for their community. In order
to evaluate the eectiveness of the campaign, the state contracted with an evaluator to work
with the local association of African-American churches to conduct an evaluation. Evaluation
components included a brief written survey of a random sample and four discussion groups
with church members. Results showed that 45% of those surveyed could recall the messages
and that the messages were most frequently heard on the radio. Discussion group results with
church members who had seen the campaign showed that 90% of them felt the messages
were appropriate for their community. Consequently, the state determined that for the next
counter-marketing campaign, they would not only implement the campaign using TV, radio
and print, but that the emphasis would be on radio spots. Additionally, to evaluate outcomes,
the state planned to include questions assessing exposure to the ads and changes in attitudes
and behavior in a subsequent population-based evaluation survey.
In analogous fashion, you can compare information on program activities with criteria for
understanding the capacity of interventions to identify and eliminate tobacco-related disparities. In
Exhibit 3-4, we provide several examples of activity and output criteria and process indicators. Again,
it is important to note that these are provided as illustrative examples only, and do not represent
programmatic guidelines from CDC on inputs, activities, outputs, criteria, or indicators.
23

Exhibit 3-3: Activities and Outputs—Comparing Indicators to Criteria
Type of
Activity
Counter-
marketing
Policy and
regulatory
action
Community
mobilization
School-based
prevention
Activity
Example Criteria Example Indicators
Implementation of a culturally
appropriate multi-channel media
campaign (TV, radio, and print)
encouraging African Americans
to develop smoke-free home and
automobile rules
Description of whether and
how counter-advertising
campaign is implemented
Collaboration with governmental
agencies and partners to
develop a comprehensive plan
to carry out smoke-free law
implementation (e.g., signage,
educating businesses)
Description of process
used to develop plan (e.g.,
identication of stakeholders,
steps taken to develop plan)
Minimum of 6 earned
media spots, quarterly press
conferences, and press releases
on current policy and regulatory
issues (e.g., taxation, secondhand
smoke policy)
Number of media spots, press
conferences/press releases,
and topics addressed
Provision of appropriate, timely
and useful technical assistance to
all local partners
Description of whether and
how technical assistance is
provided to local partners
Complete an assessment of
the existence of and perceived
compliance with tobacco-free
school policies
Description of whether
tobacco-free school policies
are in place and perceptions
of compliance
Output
Example Criteria Example Indicators
75% of African-American
adults recall the campaign
messages about secondhand
smoke exposure in homes
and automobiles and perceive
them as appropriate for their
community
Percentage of African-
Americans that recall
campaign messages
and perceive them to
be appropriate for their
community
Quality written comprehensive
implementation plan completed
in collaboration with appropriate
government agencies and
partners
Appropriate external
secondhand smoke
policy experts assess
implementation plan as
high quality
Quarterly newspaper articles
and editorials as a result of press
conferences and press releases
Frequency of articles and
editorials that reference
materials or information
provided in the press
release and/or press
conference
85% of local partners assess
technical assistance as
appropriate, timely, and useful
Percentage of local
partners that assess
technical assistance as
appropriate, timely and
useful
75% of school districts respond
to the survey of tobacco-free
school policies and data are used
to develop an action plan to
increase school district coverage
Response rate to
assessment and action
plan to increase school
coverage
Introduction to Process Evaluation in Tobacco Use Prevention and Control
24

Exhibit 3-4: Tobacco-Related Disparities: Activities and Outputs—Comparing Indicators to Criteria
Type of Activity Activity Output
Example Criteria Example Indicators Example Criteria Example Indicators
Partnership
development
Collaborative relationships
will be established with each
CDC funded National Network
to reduce tobacco related
disparities with their respective
priority population groups
Number of agreements
to work with the
National Networks
As a result of each collaboration,
one strategy and two opportunities
to reach and impact each priority
population will be identied and
assessed as culturally competent by
priority population representatives
Identied strategies and
opportunities assessed
by priority population
representatives as culturally
competent
Strategic plan
to address
disparities
A group composed of
appropriate and diverse
stakeholders will work to
develop a disparities strategic
plan
Evidence of
involvement of
stakeholders from
priority populations in
development of plan
A disparities strategic plan will be
developed and incorporated into
the overall strategic plan, along with
implementation strategies
Overall strategic plan,
including disparities plan
and implementation
strategies
Knowledge
integration
Using knowledge about
tobacco-related disparities,
two culturally competent
interventions will be
implemented with priority
populations
Priority populations
and interventions
identied
Two tailored population-based
interventions implemented as
designed reaching 40% of the
identied priority populations
Evaluation will show
implementation of the
interventions as designed
(i.e., delity) and percentage
of priority population
reached
Surveillance Develop and implement
surveillance systems that
are able to identify tobacco-
related disparities
Description of whether
and how knowledge,
attitudes, and behavior
of specic populations
can be sampled and
estimated
Data on two specic populations are
collected and analyzed
Evidence that data systems
describing tobacco-related
knowledge, attitudes, and
behavior meet professional
standards
Evaluation Conduct evaluation of quitline
promotional campaign to
reach rural populations
Evaluation of
promotional campaign
conducted
Evaluation completed and used
to inform decisions about how to
increase rural populations’ utilization
of the quitline
Assessment of whether and
how evaluation results were
used by decision makers to
inform decisions about the
quitline
Section 3—Information Elements Central to Process Evaluation
25

Introduction to Process Evaluation in Tobacco Use Prevention and Control
CASE EXAMPLE: PROGRAM STRUCTURE AND COMPONENTS
Implementation of the Henry J. Kaiser Family Foundation’s Community Health Promotion Grant
Program
In 1986, the Kaiser Family Foundation initiated the Community Health Promotion Grant Program to
help communities develop health interventions in one or more targeted health areas. Funded sites in 11
communities in the western United States received grants of up to $450,000 and were given great exibility
in developing and implementing intervention activities that were appropriate for their communities.
Grantees were asked to: (1) establish a coalition with a broad range of community agencies and organizations,
(2) conduct a formal needs assessment, and (3) address one or more of the ve targeted health issues.
How process evaluation was helpful:
Because grantees were given latitude in developing coalitions and implementing interventions, it was critical
that the research team could gather information to describe the program in each community. The type of
information collected on the program and target area included type of location (urban/suburban/rural), target
area population, community population demographics, sponsoring agency, health target areas, primary
intervention audience, impetus for the program, and a description of the primary interventions.
Advantages for you:
Findings from this component of the process evaluation revealed considerable variation across sites, in
terms of both the interventions used and the target populations. Information on program structure and
components in the various sites was critical to interpreting other ndings from the process and outcome
evaluations.
SOURCE: Wickizer TM, Wagner E, Cheadle A, Pearson D, Beery W, Maeser J, et al. Implementation of the
Henry J. Kaiser Family Foundation’s Community Health Promotion Grant Program: A process
evaluation. Milbank Quarterly 1998;76(1):121–47.
26

Section 3—Information Elements Central to Process Evaluation
CASE EXAMPLE: THEORY AND FIDELITY
New York Statewide School Tobacco Policy Review
Enactment of the federal Pro-Children’s Act of 1994 and other public health laws has prompted schools to
create policies that address the tobacco issue. However, little was known about the quality of these resulting
school policies. To assess the quality of all New York schools’ tobacco policies, the New York State Education
Department (NYSED) commissioned a systematic review. NYSED designated the Statewide Center for Healthy
Schools to lead the review of tobacco policies submitted by all New York school districts between April and
August 2001.
How process evaluation was helpful:
The Center developed a policy rubric using two guides: Fit, Healthy, and Ready to Learn and the School Health
Index. The rubric assessed ve policy components including (1) Developing, Overseeing, and Communicating
the Policy (2) Purpose and Goals, (3) Tobacco-Free Environments, (4) Tobacco Use Prevention Education, and
(5) Assistance to Overcome Tobacco Addictions. In total, 471 tobacco policies were reviewed using this rubric.
Results demonstrated that overall, policy scores were low.
Advantages for you:
The assessment demonstrated that many school districts had policies that did not provide tobacco-free
environments for students and that additional technical assistance should be provided to assist schools in
developing and enforcing eective policies consistent with CDC guidelines. In many cases it appeared that
tobacco policies were developed by outside counsel with little consideration given to developing practical
tobacco policies using input from key stakeholders and/or the larger community. These results prompted
increased eorts to provide information, training, and technical assistance to the school districts to help
improve their tobacco policies.
SOURCE: Stephens YD, English G. A statewide school tobacco policy review: Process, results, and
implications. Journal of School Health 2002;72(8):334–338.
27

Introduction to Process Evaluation in Tobacco Use Prevention and Control
CASE EXAMPLE: COLLABORATIONS AND PARTNERSHIPS
Elimination of Secondhand Smoke through the Seattle and King County Smoke-Free Housing Initiative
There is no safe level of exposure to secondhand smoke. Washington State law protects King County from
exposure in public places and the workplace; the greatest exposure thus occurs in the home. Striving for a
complete smoke-free policy means that smoking is prohibited in all private units of multi-unit housing, all
indoor common areas, and in outdoor areas, including all patios, porches, and decks and anywhere from
which smoke can drift to the inside.
How process evaluation was helpful:
The King County Tobacco Prevention Program has identied two strategies to promote smoke-free policies in
housing: regulatory and voluntary.
The regulatory strategy includes changing zoning codes to prohibit smoking in multifamily residential units
in King County and for Public Health to name secondhand smoke as a nuisance under Washington’s nuisance
law. Through an action of the Board of Health, smoke-free multi-unit housing could become a regulation.
Partnering with development and management companies to demonstrate the value and viability of
smoke-free housing is one tactic to inuence regulation, as well as working through the policy-development
channels within the County’s health department.
The voluntary strategy is to assist property managers, landlords, and condominium boards to introduce
smoke-free policies with education and technical assistance and to empower tenants to work with the
property decision-makers. Tactics include increasing tenant awareness, using targeted and broad-scale media,
conducting outreach with the largest owners of multi-unit housing, and partnering with rental associations to
provide education and tools.
Each tactic contains specic measurables (e.g., number of partnerships, training attendees, quantity and
quality of media). Collecting this process evaluation information by monitoring progress made will help
determine which activities are fruitful and worth more investment, and which goals may need a dierent
approach.
Advantages for you:
Careful monitoring of each of a program’s intermediate objectives, with corresponding recording of
achievements -- such as zoning code changes, number of units smoke-free -- enables you to know which
tactics better lead to accomplishment of desired outcomes.
SOURCE: Public Health, Seattle and King County Smoke Free Housing Initiative, Tobacco Prevention
Program (Brochure, 2006).
28

Section 4—Managing Process Evaluation
4. MANAGING PROCESS EVALUATION
As noted in the Introduction, there is no single right way to design and conduct process evaluations. The
following chapter provides an overview of critical evaluation standards, and practical procedures for managing
evaluation.
11
These fundamental components are intended to provide a foundation for eective utilization-
focused, participatory evaluation design and implementation. Information on managing evaluation has been
included to provide practical guidance on clarifying roles and responsibilities as you work with consultants and
stakeholders throughout the evaluation process.
Although the following 10-step process identies general stages of the evaluation process, claries roles, and
suggests realistic time horizons for completing each stage of an evaluation, the process is not prescriptive
regarding the methods and content of the evaluation. The model is exible: it can be adapted to the local
context, and used for both process and outcome evaluations. While it may not be necessary for every evaluation
study, a primary benet of the process is that it ensures that program sta and evaluators work together with
stakeholders.
4.1 Managing Process Evaluation: A 10-Step Process
Although the conceptual information provided in the previous sections is useful in framing and directing an
approach to evaluation, it does not provide practical guidance on how to apply these concepts in the day-to-day
management of evaluation. Program managers often ask questions such as these:
• How do you manage an evaluation of a large state government program?
• Why have an evaluation advisory group? Who should be on it?
• How do you coordinate an evaluation of programs at the community level?
• What are the dened roles of evaluation sta and stakeholders?
• How can the program manager work eectively with the evaluation sta and stakeholders?
• How do you identify which sta should be involved?
• How do you work eectively with external evaluation consultants?
4.1.1 Purpose: Why Use the 10-Step Process for Managing Evaluation?
One issue faced by tobacco control managers in conducting evaluation is identifying an appropriate evaluator.
It can be challenging to identify an evaluator who is comfortable with a participatory model for conducting
evaluation and accepts the Joint Committee Evaluation Standards (See Section 4.2). This process has been
designed as a way of operationalizing the utilization-focused approach to evaluation, which posits that the
primary criterion for judging an evaluation should be its use.
8
As noted in the Introduction of this manual,
process evaluations can be used for program improvement, monitoring, and accountability. However, to ensure
29

Introduction to Process Evaluation in Tobacco Use Prevention and Control
that information collected, analyzed, and reported meets the needs of all stakeholders, you should work with the
people who will be using this information from the beginning of the evaluation process, and focus on how they
will use it.
The 10-step process for managing evaluation helps program managers and evaluators address questions like
those posed above. It is a practical and usable approach that clearly denes the roles and responsibilities of
the program manager (or designee) and the evaluator as they work closely with an advisory group of primary
intended users and stakeholders.
12
This process was eld tested for ve years and provides a practical approach
to process evaluation.
12
The process involves an evaluation advisory group, an evaluation facilitator (typically the program manager
or designee), and the evaluator (internal sta or an external consultant). The 10-step process builds evaluation
capacity in program sta by creating a common understanding of evaluation and a systematic process for
designing and implementing it.
It also enhances the evaluator’s ability to engage stakeholders and collaboratively plan and implement a
utilization-focused evaluation.
10
The process increases the likelihood of the evaluator producing a useful report
by working with the evaluation advisory group to conceptualize the study, develop the evaluation questions,
and assist in the interpretation of the data.
4.1.2 Roles of the Advisory Group, Evaluation Facilitator, and Evaluator
An overview of the roles of the evaluation advisory group, the evaluation facilitator, and the evaluator in
the 10-Step process is presented below. Appendix C provides additional details on the evaluation advisory
group, including the benets of establishing one, selection of group members, and further details on the
responsibilities of the advisory group.
Role of the evaluation advisory group: The advisory group’s function is to provide input throughout the
evaluation, to help the evaluator think through various program issues, to review drafts of the evaluation plan
and data collection instruments, to provide insights into the collected data, and to make recommendations
based on the evaluation’s ndings. The group’s role is a reective one, not one of making nal decisions about
the evaluation’s design, implementation, or nal report. In addition, the advisory group provides insights into
the social and/or political context of the program being evaluated, which often accounts for the variation in how
programs are implemented.
Role of the evaluation facilitator: The evaluation facilitator plays a central role throughout the 10-step process.
In general, facilitators manage the relationship between the evaluation advisory group and the evaluator,
help to select an appropriate evaluation design, garner organizational and political support to implement the
evaluation, provide technical and logistical assistance, and facilitate the use of the evaluation results among
primary intended users and program stakeholders. Managing these relationships is crucial to ensure that the
input and feedback provided by the advisory group is reected in the evaluation design and implementation.
30

Section 4—Managing Process Evaluation
The evaluation facilitator also plays a critical role in building organizational capacity to conduct evaluation
by identifying and selecting an appropriate evaluator, as well as working with the evaluator to provide a
comprehensive introduction to key evaluation concepts, as needed, to the advisory group.
Either the program manager or a designee who is integrally involved in the programmatic aspects of the
intervention and/or program should serve as the evaluation facilitator. The evaluator should not serve as
both evaluation facilitator and evaluator because it will likely diminish the benets of the 10-step process and
will increase the risk that the evaluation is designed without meaningful programmatic insight, which could
ultimately reduce capacity for evaluation and negatively impact use of evaluation results.
Role of the evaluator: The evaluator is responsible for making nal decisions on the evaluation’s design, data
collection instruments, data collection methods and procedures, data analysis, and writing of the nal report.
While there may be issues that the evaluator needs to negotiate with the advisory group, the evaluator is
ultimately responsible for carrying out the evaluation in an eective, ethical, and professional manner.
4.1.3 Stages and Steps of the 10-Step Process
The 10-step evaluation process provides a protocol for participants to follow that outlines each step in four
stages: groundwork, formalization, implementation, and utilization. An overview of the four stages of the 10-step
process and the suggested timeline for a 12-month evaluation are presented in Exhibit 4-1. The timeline can be
adjusted to the local context as needed. For example, when evaluating a two-year project, the implementation
phase could take longer than is presented in Exhibit 4-1.
31

Introduction to Process Evaluation in Tobacco Use Prevention and Control
Exhibit 4-1: Overview of the 10-Step Process for Managing Evaluation
Stage Steps
I. Groundwork
In this stage, the evaluation plan is drafted, with attention to how the
evaluation process and ndings will be used in decisions about policy and
programmatic modication or termination. The study’s purpose, questions,
and methods is determined during this stage.
1–3
(Approximately 11 weeks)
II. Formalization
In this stage, the formal agreements, supporting infrastructure, and details
of implementation are negotiated and agreed on. This stage includes
development of the proposal and data collection instruments and
compliance with IRB policies (and OMB for federal institutions), if applicable.
4–5
(Approximately 11 weeks)
III. Implementation
In this stage, the program evaluation is conducted and data collection
and preliminary analyses are completed. Special attention is given to early
ndings and possible recommendations. Then, a draft report is prepared and
there is further formalization of the study’s ndings and potential resulting
recommendations. The draft report is reviewed by the evaluation advisory
group, and the report is nalized with their input.
6–8
(Approximately 23 weeks)
IV. Utilization
9–10
In this stage, the ndings are translated into decisions for action.
(Approximately 7 weeks)
Detailed information on all ten steps of the process, as well as the responsibilities and activities of the evaluation
facilitator and the evaluator for each step, are presented in Exhibit 4-2. The responsibilities and activities of the
evaluation advisory group at various steps throughout the process are also specied.
32
Section 4—Managing Process Evaluation
Exhibit 4-2: Steps and Sta Responsibilities in the 10-Step Process
STAGE I. GROUNDWORK
Role of Evaluation Facilitator Role of Evaluator
STEP 1: Identify evaluation project and evaluator
a. Meets with key program sta to identify priority
evaluation topic
b. Identies external consultant or in-house evaluator
STEP 2: Conference call or meeting with key sta and evaluator
a. Schedules conference call or meeting with key sta and
evaluator to discuss basic information needed to plan
the evaluation (e.g., purpose; logic model; identication
of intended users, uses, and stakeholders)
Participates in conference call or
meeting
STEP 3: Collaboration with advisory group to plan the evaluation
a. Identies evaluation advisory group Assists with identication of a
diverse advisory group
b. Schedules meeting or call with the advisory group and
the evaluator (minimum of 2 hours) to get input on:
• purpose/uses of the evaluation
• users of the evaluation
• evaluation questions
• methodologies
• political considerations
Participates in meeting
STAGE II. FORMALIZATION
STEP 4: Proposal and data collection instruments are drafted, distributed, and reviewed
a. Drafts proposal and data collection
instruments (e.g., written surveys,
telephone surveys, personal/group
interviews)
b. Reviews draft proposal and data collection instruments
with program manager and recommends changes if
necessary; approves proposal, instruments, and plan for
participant protection
c. Once approved by program manager, distributes plans
to evaluation advisory group for 2-week review
d. Collects feedback on proposal and data collection
instruments from evaluation advisory group and
forwards to evaluator
(Continued)
33

Introduction to Process Evaluation in Tobacco Use Prevention and Control
Exhibit 4-2: Steps and Sta Responsibilities in the 10-Step Process (continued)
STAGE II. FORMALIZATION (continued)
Role of Evaluation Facilitator Role of Evaluator
STEP 5: Proposal and data collection instruments revised, nalized, and submitted for IRB approval;
contract signed if using external evaluator
a. Approves nal proposal and data collection instruments
with program manager
Finalizes proposal and data
collection instrument/works to
comply with IRB process
b. Ensures appropriate sta sign proposal, which is
attached to contract if using an external evaluator
Signs proposal
STAGE III. IMPLEMENTATION
STEP 6: Data collection, entry, and analysis
a. Collects, enters, and analyzes data;
prepares preliminary ndings;
sends ndings to evaluation
facilitator
b. Reviews preliminary ndings/shares with program
manager
STEP 7: Preliminary ndings are shared with evaluation advisory group
a. Distributes ndings to evaluation advisory group
b. Schedules call or meeting with evaluation advisory
group to discuss ndings and identify format for
reporting ndings
Participates in evaluation advisory
group meeting
STEP 8: Draft report prepared, distributed, reviewed, and nalized
a. Prepares draft report
b. Reviews report and shares with program manager
c. Once approved by program manager, distributes to
advisory group for 2-week review
d. Collects feedback from advisory group and forwards to
evaluator
e. Finalizes report
STAGE IV. UTILIZATION
STEP 9: Meeting to wrap up evaluation study and discuss utilization of ndings and dissemination of
report(s)
a. Schedules meeting with evaluator to review the
evaluation process and discuss how the evaluation can
be used, and if appropriate, the development of the next
evaluation
Participates in meeting
b. Disseminates report to intended users/stakeholders and
others
(Continued)
34

Section 4—Managing Process Evaluation
Exhibit 4-2: Steps and Sta Responsibilities in the 10-Step Process (continued)
STAGE IV. UTILIZATION (continued)
Role of Evaluation Facilitator Role of Evaluator
STEP 10: Development of action plan for use of the evaluation
a. Develops action plan with program manager for
implementation and monitoring
Participates as appropriate
b. Continues evaluation process; targets area for evaluation
from rst year or identies new priority topic for
evaluation
4.1.4 Further Guidance on Implementing the 10-Step Process
Considerations for Stage I: Stage I activities focus on engaging the evaluation advisory group and developing
a feasible evaluation plan. However, the very rst step is to identify exactly what program or intervention will be
evaluated. Tobacco control programs are complex, multi-component systems that include community coalitions,
policy directives, mass media campaigns, and telephone quitlines, among other activities. The following criteria
will help you identify projects or program activities that will increase your ability to complete a useful evaluation:
• The selected program/intervention should be signicant and of importance to tobacco use prevention
and control. It should be of sucient importance that the process evaluation and report will be seriously
reviewed in policy and program decisions.
• It should provide practical questions to address.
• Sta should be motivated to do process evaluation on the topic.
• The process evaluation must provide data that address the questions being asked by the program sta/
stakeholders.
• There must be agreement that the program can be evaluated within the agreed upon cost and time frame.
• The process evaluation should be sensitive to the interests of a wide range of tobacco use prevention and
control stakeholders.
• When possible, data should be collected that will allow decisions to be made on dierent levels (e.g.,
program decisions, management decisions).
• The data produced must be useful for decision making.
If needed, evaluation advisory group members should be provided with a brief introduction to the fundamentals
of evaluation prior to the initial advisory group meeting. Two potential resources include Introduction to Program
Evaluation in Comprehensive Tobacco Control Programs
2
and Utilization-Focused Evaluation.
8
Orienting advisory
group members in this way will foster their participation in the process and enhance the capacity for evaluation.
It will also prepare advisory group members to assist with identifying primary evaluation uses, prioritizing key
evaluation questions, and assessing appropriate data collection methods. Ideally, the evaluation facilitator and
the evaluator will participate in this introduction as a way to build rapport with advisory group members.
35

Introduction to Process Evaluation in Tobacco Use Prevention and Control
The initial advisory group meeting (Step 3b) is a critical milestone in the evaluation. Eectively engaging the
advisory group in the evaluation planning will set the stage for continued success throughout the evaluation
process. Careful preparation should be made to ensure the active participation of all advisory group members in
critically assessing the core components of the evaluation plan.
One challenge that often arises during the rst evaluation advisory group meeting is that more evaluation
questions are identied than can be answered within the timeframe and resources available to conduct the
study. When this occurs, advisory group members must prioritize the identied evaluation questions. Failure
to do so can result in an inability to adequately answer the most useful evaluation questions within resource
limitations.
Considerations for Stage II: Stage II activities include formalizing the process evaluation plan. Ideally, the
nal plan will be included as part of the statement of work in the formal contract if an outside evaluator is
used. However, you may nd it necessary to nalize the evaluator contract prior to beginning any work on the
evaluation. If so, it is best to be as explicit as possible in the request for proposals and the statement of work
with the evaluator regarding the use of a participatory process to be used when developing and completing
the evaluation. Explicitly telling the evaluator that it is required to eectively engage primary evaluation users
throughout the evaluation project will help avoid frustration. Too often, contractors work independently of the
program sta and primary intended evaluation users, and may fail to meet the program evaluation standards
(See Section 4.2.1); and this often results in a nal report with little to no information useful for program
improvement, monitoring, or accountability purposes.
Considerations for Stage III: Stage III, evaluation implementation, takes the longest amount of time to
complete. Implementation involves data collection and analyses, as well as meetings with the evaluation
advisory group to help interpret the ndings. This latter component is critical because the advisory group will
have valuable insight into programmatic issues that drive the results.
The evaluation advisory group will also play a critical role in determining the best format for reporting results
that will be used in program decision making. Historically, evaluations culminate in a lengthy nal report that
uses standard scientic research principles to report methodology, ndings, and conclusions. Unfortunately, this
formal report often becomes a barrier to practical use of the evaluation information. You should work with the
evaluation advisory group to identify the most eective ways to report evaluation information and the optimal
timeline for release of this information to overcome this barrier, recognizing that multiple reports may be
needed for dierent audiences. The format and timeline for reporting process evaluation information should be
driven by the primary purpose and planned uses of the evaluation. For example, process information collected
to improve the program must be available quickly to maximize its use in making midcourse changes and
improvements. Clarifying the form and structure for communicating evaluation information will be an iterative
process based on the changing needs of the primary evaluation users. Because advisory group members
represent the primary users of the evaluation information, the advisory group is the best source of guidance on
form and function of the summaries within the given context of the program. Following are some alternative
formats for reporting evaluation results:
13
36

Section 4—Managing Process Evaluation
• Short communication (memo, fax, e-mail)
• Personal discussions with stakeholders
• Interim/progress reports
• Executive summaries
• Chart essays
• Verbal presentations
• Newsletters, bulletins, and brochures
• Videotape presentations
• Poster presentations
• Public meetings
• News media communication
Considerations for Stage IV: Stage IV includes utilization of evaluation information and dissemination of
evaluation ndings to primary stakeholders. During this stage, evaluation ndings and recommendations are
translated into implementation decisions.
12
Note that creation of the dissemination plan is a distinct process
from development of an evaluation plan.
Tailoring the 10-step process: The process was designed to be completed in approximately 12 months.
However, the process is adaptable to local context and to studies of dierent lengths. For example, a study can
be implemented for 6, 12, or 18 months using the same framework by adjusting the time frames for each stage.
This process can also be used with an expert panel that is convened to identify the evidence base for the
program, and to provide guidance to the development of a logic model. The inclusion of select expert panel
members on the advisory committee can contribute a valuable perspective to practical concerns such as
evaluation questions, methods, and use.
4.2 The Program Evaluation Standards and Protecting Participants in Evaluation
Research
4.2.1 The Program Evaluation Standards
The Program Evaluation Standards of the Joint Committee on Standards for Evaluation
14
outline a set of utility,
feasibility, propriety, and accuracy standards that will help you to develop and implement an ethical, useful
process evaluation that makes the best use of limited resources. (See Appendix B for more information.) As you
identify evaluators to assist with the design and completion of your process evaluation, you should make sure
37

Introduction to Process Evaluation in Tobacco Use Prevention and Control
that they are familiar with and hold themselves accountable to these professional standards. Additionally, when
the 10-Step Process for Managing Evaluation is used, the evaluation facilitator, evaluator, and evaluation advisory
group should be familiar with the standards and agree that the evaluation will conform to them.
The standards are designed to ensure that the evaluation follows four overarching principles:
1. Utility: The evaluation will serve the information needs of intended users.
2. Feasibility: The evaluation will be realistic, prudent, diplomatic, and frugal.
3. Accuracy: The evaluation will reveal and convey technically adequate information about the features
that determine worth or merit of the program being evaluated.
4. Propriety: The evaluation will be conducted legally, ethically, and with due regard for the welfare of
those involved in the evaluation, as well as those aected by its results.
4.2.2 Protecting Participants in Evaluation Research
Investigators conducting research studies that require contact with human subjects (e.g., surveys, focus group
discussions) typically must receive Institutional Review Board (IRB) approval. However, a program evaluation
intended to gather information solely for improving that program (as opposed to producing generalizable
knowledge) is not necessarily considered research. Non-research studies do not necessarily need IRB review.
Whether IRB review will be required depends on the local context. Program managers should check with their
institution’s IRB before starting evaluation studies to determine whether IRB approval will be required. IRB
reviews take time, so this determination should be made as early as possible.
IRBs review study protocols to ensure that they comply with standards for protection of human subjects.
2
When
IRB approval is required by an institution, the requirement also pertains to the institution’s contractors on the
study. If an institution lacks an IRB, it is possible to request review by an IRB at another institution. IRBs that are
registered as agreeing to follow federal policy on human research subject protection are listed at http://ohrp.cit.
nih.gov/search/asearch.asp#23ASUR.
Federal government institutions are also subject to requirements of the Paperwork Reduction Act. This Act
prohibits federal entities from engaging in systematic data collection from more than nine individuals or
institutions without approval from the U.S. Oce of Management and Budget (OMB). This requirement applies
regardless of whether the information is being collected for evaluation or research purposes.
2
For more information, see http://www.hhs.gov/ohrp/policy/index.html.
38

Section 4—Managing Process Evaluation
4.3 Choosing a Process Evaluation Design (Methodology)
The evaluator works with the advisory group to select the best data collection method for the given purpose
of the process evaluation. Evaluation data can be quantitative (i.e., quantiable, numerically expressed
information), qualitative (i.e., information in a narrative format), or a combination of both. Quantitative methods
generally use standardized instruments to collect data, which are transferred into numerical values and analyzed
using statistical methods. Collection and analysis of quantitative data is often perceived to be more objective.
However, quantitative data often lack the richness of information provided by qualitative methods.
Qualitative methods are appropriate for the collection of detailed descriptions of processes and for program
accountability, monitoring, and improvement. Specically, process data can provide detailed information on
how a program operates, whether it is operating as expected, and what program elements are more (or less)
successful. Formative evaluations focusing on program improvement often use process data.
15
Qualitative
methods typically provide stronger evaluation tools (1) when there is uncertainty as to why a program
component or intervention is or is not working or (2) when the evaluator is searching for unidentied variables.
Open-ended qualitative data, unrestricted by predetermined categories, are often used in process evaluations
because these data can provide detailed answers to complex issues not yet understood by the evaluator
or program manager. This type of data collection method “emphasizes understanding, rather than precise
measurement, of events”; it is a dynamic process where evidence can be gathered using multiple perspectives.
16
The data collection is geared toward understanding processes aecting program sta and participants.
Regardless of the data collection method used, the evaluator needs to take the following six issues into account
when identifying which measurement tools to use:
9
1. Type of data collection required.
2. Frequency of data collection.
3. Persons responsible for data collection.
4. Reliability (degree to which an instrument provides a consistent rating) and validity (degree to which an
instrument measures what it is supposed to) of the data collection measures.
5. Cost.
6. Potential burden to participants and sta members.
The evaluator should discuss these issues with the program manager to identify the most appropriate data
collection tool(s).
3
Some common qualitative research methods used in process evaluation are:
17
• Case studies;
• Structured or semi-structured interviews with or self-administered surveys of program stakeholders to
gather information on program activity facilitators and barriers;
3
For additional ideas regarding evaluation methodology for tobacco programs, and for links to websites with practical
evaluation tools, consult the Tobacco Technical Assistance Consortium – www.ttac.org.
39

Introduction to Process Evaluation in Tobacco Use Prevention and Control
• Focus groups with participants, sta, or informants to generate information on the program’s design or
suggestions for program improvement;
• Direct observation to record participant and project sta behavior during an intervention; and
• Recorded reviews of minutes from program meetings, progress reports from subcontractors, self-report
inventories, diaries, or project archives.
A variety of tools can be used to analyze and interpret qualitative data. Two commonly used software programs
4
are NVivo7
18
and ATLAS.ti.
19
For example, ATLAS.ti allows the analysis of electronic text, images (e.g., scans of
handwritten notes), video (e.g., television counter-marketing advertisements), and audio (e.g., radio counter-
marketing, digitized interviews).
Two quantitative research methods are:
• Conducting surveys to measure participants’ understanding of the program or identify the source of a
program’s problem; and
• Tracking data in the form of record reviews to count the number of items distributed or collected, such
as program logs measuring the number of brochures distributed, smoke-free home pledges distributed/
received, number of people contacted or reached by the project, and number of training sessions held.
As you consider data collection method(s), it is critical to involve the evaluation advisory group to determine
which methods are feasible. The evaluator should act as a consultant to ensure that the evaluation methodology
is as strong as possible; successful programs cannot be proven eective without a defensible evaluation.
Note that much process evaluation information comes from the documents and records that programs
typically create as a part of normal operations. It is rarely necessary to construct completely new data collection
procedures in order to do process evaluation, even though it may be necessary to take steps to ensure that
existing data collection procedures are formalized for accuracy and completeness.
So, for example, information on inputs may appear in descriptive materials, approved budgets, board minutes,
inter-agency agreements (which specify partners and roles), and other documents. Information on the types of
activities for programs will often appear in strategic plans, work plans, sta logs, and inter-agency agreements.
Outputs are typically documented through work logs, participation records, and sometimes expenditure records
and accounting reports.
4
Use of trade names is for identication only and does not imply endorsement by the Centers for Disease Control and
Prevention or the U.S. Department of Health and Human Services.
40

Section 4—Managing Process Evaluation
4.4 Process Evaluation—Beyond a Single Study
You may use the steps and techniques described in this section for a single evaluation. However, you will most
likely conduct multiple process evaluations, either simultaneously or sequentially. This will require ongoing
commitment to evaluation (process and outcome) and ongoing allocation of resources. Optimally, it will also
include ongoing use of evaluation information for the purposes of program monitoring, program improvement,
development of eective program models, and accountability (as described in Section 2).
Participatory models of evaluation that engage stakeholders to serve in advisory roles (like the 10-step process
described in Section 4.1) enhance the use and applicability of evaluation information.
20
The participatory
approach builds an appreciation, knowledge, and acceptance of evaluation among those people and
organizations that participate in the evaluation process. This, in turn, encourages the use of evaluation
information in everyday program decision making. As you do more and more participatory evaluations, using
the process just described, you will increase the capacity of your organization both to carry out eective
program evaluation and to use evaluation ndings routinely.
21
You may nd it useful to have someone in your organization focus beyond the process, completion, and
timely use of any single evaluation study. This person or group could review what each discrete study has
accomplished, build on the learning acquired from each study, and work to create and sustain organizational
structures and processes to implement and use evaluation. Evaluation capacity building is a worthwhile process
to increase the likelihood of quality evaluation becoming a regular and routine part of your organization’s work.
21
41

Conclusion
5. CONCLUSION
Process evaluation is an important part of identifying ways to improve your program, monitor program
implementation, build eective program models, and demonstrate accountability. Used in coordination with
outcome evaluation, process evaluation enables you to better focus your time and resources where they will
have the greatest benet. In the ever-changing landscape of tobacco use prevention and control, systematic
collection of process information over time will help you eciently modify program components and activities
as needed. This ability to eectively compensate for changing external environments and priorities will increase
your capacity to address the health consequences of tobacco use and to justify program funding.
The remainder of this document contains references, a glossary of terms, and ve appendices covering CDC’s
framework for program evaluation (Appendix A); the program evaluation standards of the Joint Committee on
Standards for Evaluation (Appendix B); detailed information on purpose, selection, and role of the evaluation
advisory group (Appendix C); and examples of evaluation questions related to the Center for Tobacco Policy
Research’s logic model (Appendix D).
43

Glossary of Terms
GLOSSARY OF TERMS
Activities: The actual events or actions that take place as a part of a program.
Evaluation plan: A written document describing the overall evaluation approach or design. The plan describes
what will be done, how it will be done, who will do it, when it will be done, why the evaluation is being
conducted, and how the ndings will likely be used.
Indicator: A specic, observable measure of an input, activity, output, or outcome of a program.
Infrastructure: All the components necessary to conduct an evaluation (e.g., experienced sta, adequate
funding).
Inputs: Resources used to plan and set up a program.
Logic model: A systematic and visual way to present the perceived relationships among the resources you have
to operate the program, the activities you plan to do, and the results you hope to achieve.
Objectives: Quantiable statements describing the results to be achieved and the manner in which these results
will be achieved. Objectives should be specic, measurable, achievable, relevant, and time-bound.
Outputs: The direct products of program activities; immediate measures of what the program did.
Outcomes: The results of program operations or activities; the eects triggered by the program, for example,
policy or environmental changes at the state, community, or organizational level. At the individual level,
outcomes might include changes in knowledge, skills, and attitudes or changes in behaviors such as tobacco
use.
Outcome evaluation: The systematic collection of information to assess the impact of a program, present
conclusions about the program’s merit or worth, and make recommendations about future program direction or
improvement.
Priority population: A specic population experiencing tobacco-related disparities that your program has
identied for focused programmatic eorts.
Process evaluation: The systematic collection of information to document and assess how a program is
implemented and operates. This information can help determine whether the program is being implemented as
designed and can be used to improve the delivery and eciency of the program.
Program evaluation: The systematic collection of information on a program’s inputs, activities, and outputs, as
well as the program’s context and other key characteristics.
Reach: The absolute number, proportion, and representativeness of persons who are exposed to or participate
in a given program or intervention. Representativeness refers to whether participants have characteristics that
reect the target population.
Social Ecological Model: A framework for understanding health behavior change. There are ve levels at which
change can occur: individual, interpersonal, organizational, community, and society.
Stakeholder: The persons or organizations that have a vested interest in what will be learned from an evaluation
and what will be done with the information.
2
Surveillance: The monitoring of tobacco-related behaviors, attitudes, and health outcomes at regular intervals
of time.
Utility: The extent to which an evaluation produces reports that are disseminated to relevant audiences, inform
program decisions, and have a benecial eect.
Utilization-focused evaluation: A process for making decisions about critical evaluation issues, including
purpose, design, and type of data to collect. The process involves collaboration with an identied group of
primary users to determine their intended uses of evaluation ndings.
8
45

Appendix A
APPENDIX A:
CDC’S FRAMEWORK FOR PROGRAM EVALUATION
4
Step 1: Engage stakeholders. The rst step of the Framework involves identifying and engaging stakeholders
to ensure that the perspectives and needs of the primary users of evaluation information are taken into account.
Stakeholders are those people who have a vested interest in what will be learned from the evaluation and how
the evaluation ndings will be used. Stakeholders may include those involved in program operations, those
participating in or aected by the program, and other primary users of the evaluation. The level of stakeholder
involvement will vary from program to program; for example, stakeholders may provide input to the evaluator,
they may help design the evaluation, and/or they may help collect the evaluation data.
Step 2: Describe the program. Describing the program helps to ensure that all parties agree on the denition
and purpose of the program before undertaking an evaluation. A clear program description helps articulate
program goals and objectives and facilitates comparisons with similar programs. A complete program
description should include need, expected eects, activities, resources, stage of development, context, and logic
model.
Step 3: Focus the evaluation. Focusing the evaluation involves working with stakeholders to prioritize
evaluation questions and ensure that the evaluation design adheres to the standards for evaluation while
making the most ecient use of time and resources. The key areas to consider when focusing the evaluation
include purpose, users, uses, questions, methods, and agreements.
Step 4: Gather credible evidence. All information collected to conduct the evaluation must be useful, credible,
and relevant to the key stakeholders and should provide a well-rounded assessment of the program to ensure
that the evaluation addresses the program’s key purposes. Credible evaluation evidence helps ensure the utility
of the ndings and the applicability for stakeholders and others interested in learning from the evaluation. To
enhance credibility, carefully consider the indicators, data sources, quality, quantity, and logistics of gathering
evidence. Balancing the accuracy and feasibility of evaluation data often becomes a challenge that should be
addressed in collaboration with key stakeholders.
Step 5: Justify conclusions. The evaluation conclusions should be clearly linked to the evidence gathered
during the program evaluation. Given their critical understanding of the context of the program, key
stakeholders should play a primary role in interpreting evaluation evidence that will justify the evaluation
conclusions. Justication of conclusions requires close adherence to standards. This step also includes analysis
and synthesis of evaluation evidence, informed interpretation and judgment by key stakeholders, and
development of recommendations to inform program decision makers.
Step 6: Ensure use and lessons learned. Eective evaluation requires time, eort, and resources. Given these
investments, it is critical that the evaluation ndings be disseminated appropriately and used to inform decision
making and action. Once again, key stakeholders can provide critical information about the form, function, and
distribution of evaluation ndings to maximize their use.
47

Appendix B
APPENDIX B:
DETAILED LIST OF THE JOINT COMMITTEE ON STANDARDS FOR
EVALUATION: THE PROGRAM EVALUATION STANDARDS
14
Propriety Standards
The propriety standards are intended to ensure that an evaluation will be conducted legally, ethically, and with
due regard for the welfare of those involved in the evaluation, as well as those aected by its results.
P1 Service orientation: Evaluations should be designed to assist organizations to address and eectively serve the
needs of the full range of targeted participants.
P2 Formal agreements: Obligations of the formal parties to an evaluation (i.e., what is to be done, how, by whom,
when) should be agreed to in writing, so that these parties are obligated to adhere to all conditions of the
agreement or formally renegotiate commitments.
P3 Rights of human subjects: Evaluations should be designed and conducted to respect and protect the rights and
welfare of human subjects.
P4 Human interactions: Evaluators should respect human dignity and worth in their interactions with other
persons associated with an evaluation, so that participants are not threatened or harmed.
P5 Complete and fair assessment: The evaluation should be complete and fair in its examination and recording of
strengths and weaknesses of the program being evaluated so that strengths can be built on and problem areas
addressed.
P6 Disclosure of ndings: The formal parties to an evaluation should ensure that the full set of evaluation ndings,
along with pertinent limitations, are made accessible to the persons aected by the evaluation and any others
with expressed legal rights to receive the results.
P7 Conict of interest: Conict of interest should be dealt with openly and honestly so that it does not
compromise the evaluation processes and results.
P8 Fiscal responsibility: The evaluator’s allocation and expenditure of resources should reect sound
accountability procedures and otherwise be prudent and ethically responsible so that expenditures are
accounted for and appropriate.
Utility Standards
The utility standards are intended to ensure that an evaluation will serve the information needs of intended users.
U1 Stakeholder identication: Persons involved in or aected by the evaluation should be identied so that their
needs can be addressed.
49

Introduction to Process Evaluation in Tobacco Use Prevention and Control
U2 Evaluator credibility: The persons conducting the evaluation should be both trustworthy and competent to
perform the evaluation so that the evaluation ndings achieve maximum credibility and acceptance.
U3 Information scope and selection: Information collected should be broadly selected to address pertinent
questions about the program and be responsive to the needs and interests of clients and other specied
stakeholders.
U4 Values identication: The perspectives, procedures, and rationale used to interpret the ndings should be
carefully described so that the bases for value judgments are clear.
U5 Report clarity: Evaluation reports should clearly describe the program being evaluated, including its context
and the purposes, procedures, and ndings of the evaluation, so that essential information is provided and easily
understood.
U6 Report timeliness and dissemination: Signicant interim ndings and evaluation reports should be
disseminated to intended users so that they can be used in a timely fashion.
U7 Evaluation impact: Evaluations should be planned, conducted, and reported in ways that encourage follow-
through by stakeholders to increase the likelihood that the evaluation will be used.
Feasibility Standards
The feasibility standards are intended to ensure that an evaluation will be realistic, prudent, diplomatic, and
frugal.
F1 Practical procedures: The evaluation procedures should be practical to keep disruption to a minimum while
needed information is obtained.
F2 Political viability: The evaluation should be planned and conducted with anticipation of the dierent positions
of various interest groups so that their cooperation may be obtained and so that possible attempts by any of
these groups to curtail evaluation operations or to bias or misapply the results can be averted or counteracted.
F3 Cost eectiveness: The evaluation should be ecient and produce information of sucient value so that the
resources expended can be justied.
Accuracy Standards
The accuracy standards are intended to ensure that an evaluation will reveal and convey technically adequate
information about the features that determine worth or merit of the program being evaluated.
A1 Program documentation: The program being evaluated should be described and documented clearly and
accurately so that the program is clearly identied.
A2 Context analysis: The context in which the program exists should be examined in enough detail that its likely
inuences on the program can be identied.
50

Appendix B
A3 Described purposes and procedures: The purposes and procedures of the evaluation should be monitored and
described in enough detail that they can be identied and assessed.
A4 Defensible information sources: The sources of information used in a program evaluation should be described
in enough detail that the adequacy of the information can be assessed.
A5 Valid information: The information gathering procedures should be chosen or developed and then
implemented in a way that ensures the interpretation arrived at is valid for the intended use.
A6 Reliable information: The information gathering procedures should be chosen or developed and then
implemented in a way that ensures the information obtained is suciently reliable for the intended use.
A7 Systematic information: The information collected, processed, and reported in an evaluation should be
systematically reviewed and any errors found should be corrected.
A8 Analysis of quantitative information: Quantitative information in an evaluation should be appropriately and
systematically analyzed so that evaluation questions are eectively answered.
A9 Analysis of qualitative information: Qualitative information in an evaluation should be appropriately and
systematically analyzed so that evaluation questions are eectively answered.
A10 Justied conclusions: The conclusions reached in an evaluation should be explicitly justied so that
stakeholders can assess them.
A11 Impartial reporting: Reporting procedures should guard against distortion caused by personal feelings and
biases of any party to the evaluation so that evaluation reports fairly reect the evaluation ndings.
A12 Meta-evaluation: The evaluation itself should be formatively and summatively evaluated against these and
other pertinent standards so that its conduct is appropriately guided and stakeholders can closely examine its
strengths and weaknesses upon completion.
Additional Resource:
Sanders JR. The Program Evaluation Standards: How to Assess Evaluations of Educational Programs. 2d ed. Newbury
Park, CA: Sage; 1994.
51

Appendix C
APPENDIX C:
ADDITIONAL INFORMATION ON THE PURPOSE, SELECTION,
AND ROLES OF THE EVALUATION ADVISORY GROUP
Why establish an advisory group?
A fundamental element in the 10-step process is inclusion and engagement of an evaluation advisory group.
This advisory group becomes critical in ensuring that the evaluation is participatory in nature.
Given that the purpose of evaluation is to provide useful information for program improvement and decision
making, the key challenge is identifying and prioritizing what information and data would be most useful.
Everything else ows from this initial determination—methods, measures, focus, analysis, and reporting. An
evaluator, acting alone, may miss some important and relevant issues. Key stakeholders that are connected with
a program at dierent levels and in various ways can provide dierent perspectives on what is important and
useful to know. By bringing these perspectives together to inform the evaluation, each person in a collaboration
makes a contribution—and each benets.
An eective method for engaging stakeholders is to create an advisory group to participate in the design and
implementation of the evaluation and to help determine what actions are needed, based on the evaluation
ndings. Increasing evaluation capacity becomes an added benet of involving an advisory group. As
stakeholders come together to discuss dierent evaluation activities and the results of data collection, they learn
how to conduct program evaluations while also learning about each other and the program being evaluated.
This experience strengthens personal relationships and increases each participant’s ability to think evaluatively
and apply what they’ve learned to future evaluation projects.
How should advisory group members be selected?
Careful consideration should be given to the selection of advisory group members. To ensure that the group
is able to function eectively, all advisory group members must agree to commit their time and energy to
attending advisory group meetings whenever possible.
The advisory group should include representatives from the following groups:
• Sta who have administrative oversight of the program;
• Sta who are responsible for the daily operations of the program;
• Current or future recipients of program services;
• Stakeholders who are diverse in terms of class, gender, and age;
• Representatives of organizations interested in the outcomes of the evaluation;
53

Introduction to Process Evaluation in Tobacco Use Prevention and Control
• Sta who will be responsible for implementing the evaluation’s recommendations and action plan; and
• Sta who have some experience with evaluation.
In selecting advisory group members, it is a good idea to involve people who bring variety in terms of their
(1) views of the program, (2) intended uses of the evaluation results, (3) positions within the organization and
community, and (4) experience with the program being evaluated. In addition, it is important that at least some
of the team members have an understanding of the politics of the organization and the program.
How many people should be on the advisory group?
The number of people on an advisory group will vary depending on the scope of the evaluation and the nature
of the program being evaluated. Typically, advisory groups composed of 5 to 10 members are sucient to create
enough synergy and dialogue to keep the process going.
What is the role of the advisory group?
The advisory group’s function is to provide advice throughout the evaluation, to help the evaluator think
through various program issues, to review drafts of the evaluation plan and data collection instruments, to
provide insights into the collected data, and to make recommendations based on the evaluation’s ndings. The
group’s role is a reective one, not one of making nal decisions about the evaluation’s design, implementation,
or nal report. In addition, the advisory group provides insights into the social and political context of the
program being evaluated.
Members should meet to discuss the background of the program and develop the evaluation’s rationale,
purpose statement, stakeholders, and key questions to be addressed. This rst meeting is critical to getting
the evaluation focused in a way that will address the decision-making needs of the stakeholders. This meeting
should be scheduled for a minimum of two hours. Although this meeting can take place via a conference call,
ideally the advisory group will meet face-to-face at least twice during the evaluation process. In between these
meetings, members may be asked to perform additional tasks.
Advisory group members should individually review the draft evaluation plan that is prepared by the evaluation
facilitator and the evaluator.
Once the data collection instruments have been developed, the members should individually review the
instruments to ensure that the key evaluation questions are addressed and the questions or items are well
constructed.
When the evaluator has completed the data collection phase and has aggregated the data, the advisory
group should be reconvened for another face-to-face meeting. During this meeting, the evaluator facilitates a
discussion of the evaluation’s ndings and engages the group in a process of analyzing the ndings. Typically,
this discussion leads to development of a set of recommendations that the evaluator will incorporate into the
nal report. This meeting may last from two to six hours, depending on the quantity of information collected
during the evaluation and the complexity of the evaluation ndings.
54

Appendix C
After the evaluation report has been written, consider establishing a task force that will develop an action plan
for implementing the evaluation’s recommendations. This task force might be composed of the same people
who served on the advisory group or it might be a combination of advisory group members and others who
have more contact with the program’s daily operations. If original advisory group members are not involved
in the task force, it is important they understand why. All group members should always be thanked for their
original participation.
55

Appendix D
APPENDIX D:
PROCESS EVALUATION QUESTIONS AND LOGIC MODEL FROM
THE CENTER FOR TOBACCO POLICY RESEARCH
This appendix includes an example of a logic model for a process evaluation provided by the Center for Tobacco
Policy Research (CTPR), Saint Louis University School of Public Health (see also Exhibit D-1 on page 71).
The CTPR evaluated a tobacco prevention and cessation initiative funded by the Missouri Foundation for Health.
One of the initiative’s strategies focused on an educational campaign to increase awareness among the general
population about the dangers of tobacco in order to help gain public support for an increase in the state’s
tobacco tax. The evaluation also addressed numerous questions about the inputs, activities, and outputs of
this initiative. Some of the questions that the evaluation was intended to answer through analysis of inputs,
activities, and outputs appear below.
Inputs
• Were the resources for the educational campaign adequate?
• Who were the collaborators for the campaign? How eective were both the existing and new
collaborations?
Activities
• What was the level of communication among stakeholders?
• Was there sucient (or eective) communication among stakeholders?
• How was the campaign developed and implemented?
• Was the education campaign prepared for (and exible enough) to respond to environmental
changes?
Outputs
• What was the reach of the grassroots education activities?
• How many advocacy committees were developed?
• How many volunteers were recruited?
• What was the geographic coverage of the campaign?
• How many people received the education messages?
• What were the responses from various audiences to the education messages?
• Were the messages appropriate for dierent audiences?
57
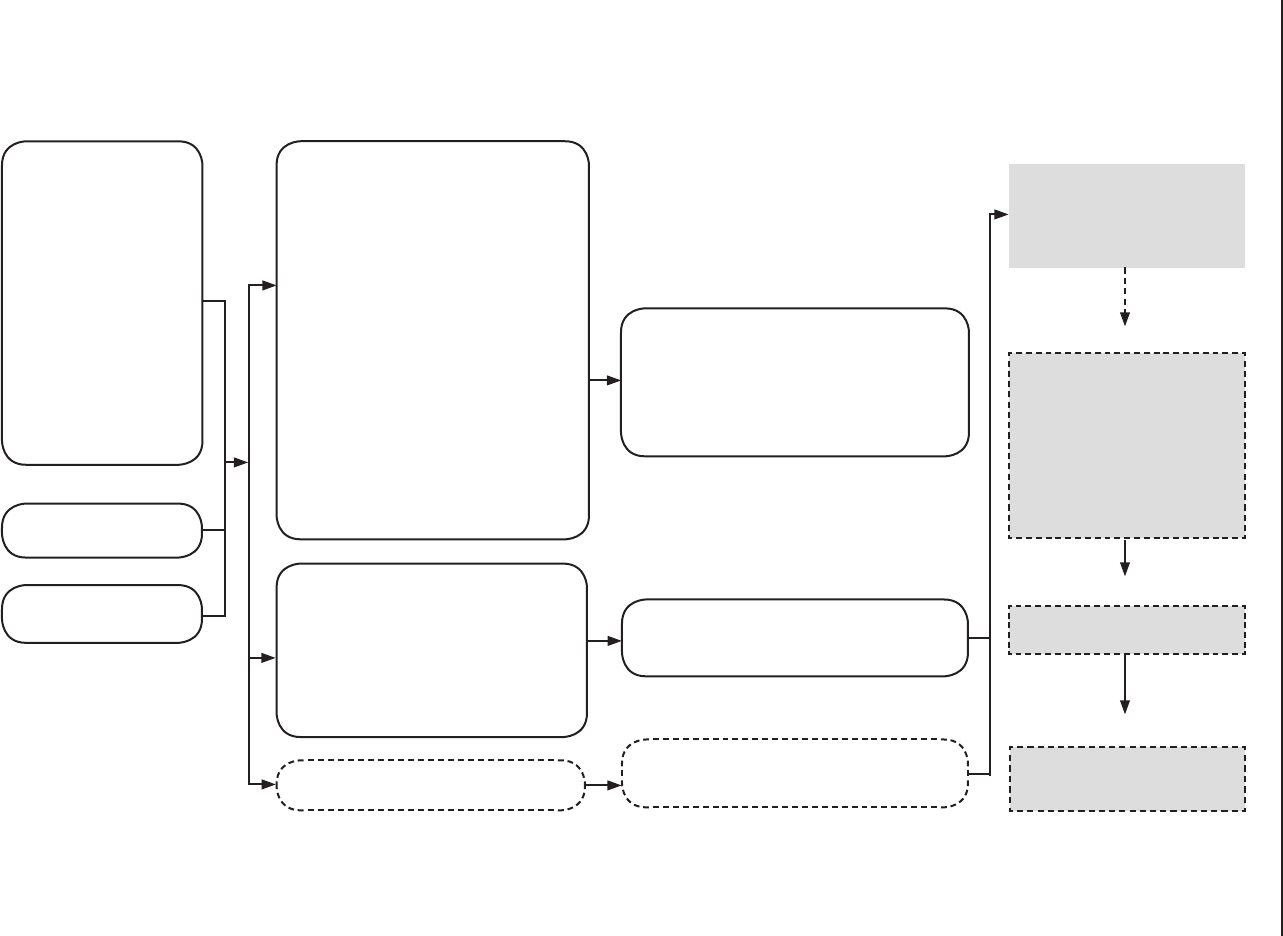
Introduction to Process Evaluation in Tobacco Use Prevention and Control
58
Exhibit D-1: Strategy 1 Logic Model: Show Me Health—Clearing the Air About Tobacco
Inputs
American Lung Association
(ALA)
ALA Funding Sources
• Missouri Foundation for
Health
• greater KC Health
Foundation
ALA Sta
• Director of Field Operations
• Regional Managers
• Kansas City
• Columbia
• Springeld
• St. Louis
• Oce Manager
• Intern
Missouri Partnership on
Smoking or Health (MPSH)
Statewide Volunteer
E orts/Grassroots
Activities
Grassroots educational campaign to
educate general public*
Details of Campaign Activities
Preparation
• Spokeperson training
• Targeting of traditional and non-traditional
partners
• Grassroots training
• Formation of advocacy committees
Outreach
• Recruitment events—presentations,
co ees, email communication
• Education events—forums, festivals, press
conferences
• Formation of advocacy committees
• Earned media campaign
• Coalition building
• Volunteer recruitment
• Written materials and communication
Public relations (Vandiver Group)
Development of message and materials
• Talking points
• Spokeperson training
• Word of Mouth Program
• Brochures
• PSAs
• Fact sheets
Polling (Nicholl Campaign)**
* Note: Funding from two of the Foundation means no
direct lobbying role for ALA sta in this educational
campaign. Advocacy is done by voluntary health
organizations and hired lobbyists.
Outputs
Grasroots Educational Campaign
1. Regional Steering Committees (goals = 5)
2. Local (city/town) Advocacy Committee (goal = 25-40)
3. Recruit 2,500+ community volunteers
4. Contact 100,000 to 200,000 people
5. Increase number of supporters to (#) through
petition/endorsement drives
Public Relations
• P
ress releases
• News stories/earned media placements (goal = 100+)
Polling **
• P
olling data on support/opposition
• Outcome indicator data for 1st short-term outcome
** Note: Funding for the Show Me Health Campaign does not go
toward polling.
Outcomes
SHORT-TERM***
• Increased knowledge of improved
attitudes toward, and increased
support for a constitutional
amendment to increase tobacco
tax.
INTERMEDIATE
1. Constitutional amendment for
increased tobacco tax placed on
the 2006 statewide ballot
2. Passage of tobacco tax increase
3. Creation of protected trust fund
Allocation of tax:
• Prevention
• Health care access
• Reserve funds
• Current tax recipient programs
LONG-TERM (beyond 2006)
• Reduced tobacco consumption
sales
IMPACT
• Reduced health care costs
• R
educed tobacco-related morbidity
and mortality
*** Note: The Show Me Health Campaign’s
involvement stops at short-term outcomes.

References
REFERENCES
1. Centers for Disease Control and Prevention. Best Practices for Comprehensive Tobacco Control Programs.
Atlanta GA: U.S. Department of Health and Human Services; August 1999.
2. MacDonald G, Starr G, Schooley M, Yee SS, Klimowski K, Turner K. Introduction to Program Evaluation for
Comprehensive Tobacco Control Programs. Atlanta, GA: U.S. Department of Health and Human Services; 2001.
3. Starr G, Rogers T, Schooley M, Porter S, Wiesen E, Jamison N. Key Outcome Indicators for Evaluating
Comprehensive Tobacco Control Programs. Atlanta, GA: U.S. Department of Health and Human Services; 2005.
4. Centers for Disease Control and Prevention. Framework for program evaluation in public health. MMWR
1999b;48(RR11):1–40.
5. Mueller N, Luke D, Herbers S, Montgomery T. The best practices: Use of the guidelines by ten state tobacco
control programs.American Journal of Preventive Medicine 2006;31(4).
6. Zaza S, Harris KW, Briss PA, editors. The Guide to Community Preventive Services: What Works to Promote Health.
Task Force on Community Preventive Services; 2004.
7. California Department of Health Services, Tobacco Control Section. Communities of Excellence in Tobacco
Control (Modules 1 and 2). Pre-production copy; September 2006.
8. Patton MQ. Utilization-Focused Evaluation: The New Century Text. 2nd edition. Newbury Park, CA: Sage; 1986.
9. Steckler A, Linnan L, editors. Process Evaluation for Public Health Interventions and Research. San Francisco, CA:
Jossey-Bass; 2002.
10. Patton MQ. The CEFP as a model for integrating evaluation within organizations. Cancer Practice 2001;9(1):
S11-S16.
11. Compton D, Baizerman M, editors. Managing Program Evaluation: Towards Explicating a Professional
Orientation and Practice. New Directions for Evaluation (forthcoming).
12. Compton DW, Baizerman M, Preskill H, Rieker P, Miner K. Developing evaluation capacity while improving
evaluation training in public health: The American Cancer Society’s Collaborative Evaluation Fellows Project.
Evaluation and Program Planning 2001;24 (1):33–40.
13. Torres R, Preskill H, Piontek M. Evaluation Strategies for Communicating and Learning: Enhancing Learning in
Organizations. Thousand Oaks, CA: Sage Publications, Inc.; 1996.
14. Sanders JR. Joint Committee on Standards for Educational Evaluation. The Program Evaluation Standards: How
to Assess Educational Programs. 2nd Edition. Thousand Oaks, CA: Sage Publications, Inc.; 1994.
15. Patton MQ. Qualitative Evaluation and Research Methods. 2nd ed. Thousand Oaks, CA: Sage Publications, Inc.;
1990.
16. Weiss CH. On theory-based evaluation: Winning friends and inuencing people. The Evaluation Exchange
2004;IX(4):1-5.
17. Mattessich P. The Manager’s Guide to Program Evaluation: Planning, Contracting, and Managing for Useful
Results. Saint Paul, MN: Amherst H. Wilder Foundation; 2003.
18. NVivo 7. QSR International, Inc.
19. Atlas.ti. Scientic Software Development GmbH.
20. Greene JC. Stakeholder participation in utilization of evaluation. Evaluation Review 1988;12:2.
21. Compton DW, Baizerman M, Stockdill SH, editors. The art, craft, and science of evaluation capacity building:
New Directions for Evaluation 2002;93.
59

ProcessCoverBack.ai 3/5/2008 10:12:25 AM
CS114921
